Downloaded 710 times
![Epidemiology
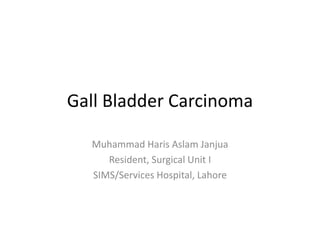
• incidence of GC 1 to 23 per 100,000 worldwide
• over the last three decades there is decrease in incidence in
developed and increase in incidence in developing countries
• The highest incidence of gallbladder carcinoma is reported more
recently from the Indian-Subcontinent including India and Pakistan
(18-23/100,000) mirror image of worldwide distribution of gall
stones
• A relatively rare malignancy worldwide but is the second
commonest gastrointestinal cancer in Pakistani women
• Most common cause of gastrointestinal cancer related mortality in
females in subcontinent.[17,18]](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-11-320.jpg)
![Epidemiology
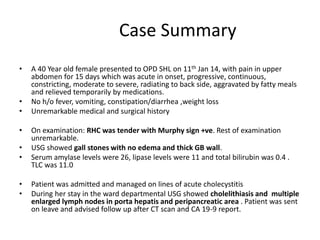
• Rise in incidence of GC from Northern India and Southern Pakistan
over the past two decades
• Frequency of gallbladder cancer in Pakistan varies between 6-7%.
[13-15]
• Highest incidence is found in Chelians, American Indian and in parts
of Northern India where it accounts for 9% of all biliary tract
diseases.
• Female to male ratio is 3:1
• Peak incidence is in 7th decade of life.[2]](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-12-320.jpg)
![Etiology/Pathophysiology
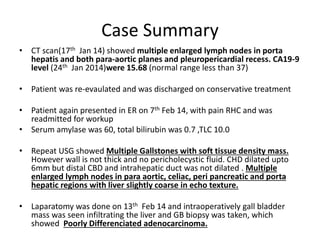
• Gallstones are present in 60-90 % of GB cancer cases (World wide)
.[3][12].
– a small proportion of patients (1-3%) with gall stones developed G.B cancer
[16,17]
– inverse relationship between the incidence of GC and rate of cholecystectomy
– In pakistan 98-100 % of cases of GC have gall stone[18][19]
• Risk factors include
– Chronic inflamation and infection.
– Porcelain Gallbladder
– Typhoid carrier
– Adenomatous polyp (size of the polyp is strongest predictor of malignant
transformation)[3]
– Advanced age(>55 yr)
– Multiparity(>5)
– Presence of gallstone larger than 1[17]-3[18]cm.
– Anomalous pancreatobiliary junction
– Drugs :OCP, methyldopa](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-13-320.jpg)
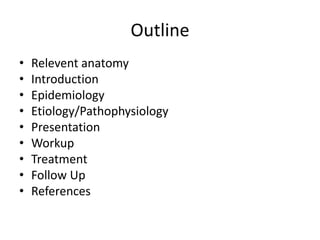
![– Occupational exposure to rubber,cigrette smoking
– Bile acid composition.
– Diet: low fibre, low calories. High fine CHO, low protein
• A 2008 study found evidence that excess body weight
in women, specifically a 5 kg/m 2increase in the body-mass
index, is strongly associated with an increased
risk of gallbladder cancer.[4]
• Numerous studies have investigated genetic
abnormalities in gallbladder cancer and have shown
that approximately 39-59% of gallbladder cancers are
associated with the K-ras mutation, while more than
90% of them are associated with a p53 mutation.[5]](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-14-320.jpg)
![Presentation
• Usually asymptomatic at the time of diagnosis
• Symptoms if present are similar to benign
diseases such as cholecystitis or biliary colic.
• Jaundice and anorexia are late features
• Palpable mass is a late sign[2]
• Given this presentation, less than 50% of
gallbladder cancers are diagnosed preoperatively.
Many are diagnosed incidentally in gallbladders
removed for biliary colic or cholecystitis.](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-15-320.jpg)

![Staging
• The American Joint Committee on Cancer (AJCC) has designated staging by the TNM (primary t umor, regional
lymph n odes, distant m etastasis) classification as follows [6]
• TNM Definitions
Primary tumor (T)
• TX - Primary tumor cannot be assessed
• T0 - No evidence of primary tumor
• Tis - Carcinoma in situ
• T1 - Tumor invades lamina propria or muscle layer . T1a - Tumor invades lamina propria
• T1b - Tumor invades the muscularis
• T2 - Tumor invades the perimuscular connective tissue; no extension beyond the serosa or into the liver
• T3 - Tumor perforates the serosa (visceral peritoneum) and/or directly invades the liver and/or 1 other adjacent organ
or structure, such as the stomach, duodenum, colon, pancreas, omentum, or extrahepatic bile ducts
• T4 - Tumor invades the main portal vein or hepatic artery or invades multiple extrahepatic organs or structures
Regional lymph nodes (N)
• NX - Regional lymph nodes cannot be assessed
• N0 - No regional lymph node metastasis
• N1 - Portal lymph node metastasis
• N2 - Distant lymph node metastasis such as periaortic, pericaval, superior mesenteric artery, or celiac artery
Distant metastasis (M)
• MX - Distant metastasis cannot be assessed
• M0 - No distant metastasis
• M1 - Distant metastasis](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-22-320.jpg)
![Non surgical Management
• Small gallbladder tumors are common and many can be safely followed
with serial ultrasonographic examination. It is generally thought that
polyps of less than 1 cm are safe to follow, although a study[7] has
recommended that polyps that are greater than or equal to 6 mm should
be considered for cholecystectomy.
• Chemotherapy is used in the adjuvant and palliative treatment of
gallbladder cancer. Phase II studies have shown that the use of single-agent
chemotherapy (with gemcitabine or 5-fluorouracil) in the palliative
setting can be beneficial.
• Combination chemotherapy also has been shown to be beneficial and is
usually based on gemcitabine, capecitabine, and 5-fluorouracil used in
combination with cis-platinum or oxaliplatinum. Fluoropyrimidine-based
chemoradiotherapy is commonly employed in the palliative and adjuvant
setting as well.](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-25-320.jpg)
![Surgical management
• Cholecystectomy recommended in
– polyps larger than 1 cm or with polyps in the setting of primary sclerosing
cholangitis
– porcelain gallbladder.[2]
• Diagnostic Laproscopy
– In order to exclude the presence of undetected intra-abdominal metastases
prior to curative laparotomy.
– Surgery is contraindicated in the presence of distant metastases.
• Exploratory Laparotomy
– The initial exploration focuses on the presence of metastatic disease that was
not detected by preoperative imaging and staging laparoscopy.(15%)
– In view of North american surgeons Biopsy-proven metastases in the celiac
nodes preclude resection.
– Aortocaval nodal metastases are considered distant metastatic disease.](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-26-320.jpg)
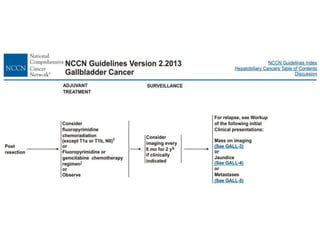
![No standard adjuvant treatment protocol has been
defined for gall bladder cancer.
– A 2008 study found that only 20% of patients with gall
bladder cancer received adjuvant treatment.[9]
– In the report, no benefit from adjuvant therapy could
be demonstrated, but only a small number of patients
received this treatment.
– Generally, fluoropyrimidine-based chemoradiotherapy
or single-agent chemotherapy with fluoropyrimidines
or gemcitabine is used.[10]
– Because of the high cure rate with surgery alone for
T1N0 lesions, adjuvant therapy is not commonly
offered to these patients.](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-31-320.jpg)
![PROGNOSIS [5][11]
STAGE 5 YEAR SURVIVAL RATE
T1b 100% especially with hepatectomy
T2 38% to 77% after extended
cholecystectomy
III and IV 25 % with extended resection
Unresectabe disease < 5% ( 1 year survival rate)
Patients with unresectable disease have a median survival of 2-4 months](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-38-320.jpg)
![References
1. D'Hondt M, Lapointe R, Benamira Z, Pottel H, Plasse M, Letourneau R, et al. Carcinoma of the
gallbladder: Patterns of presentation, prognostic factors and survival rate. An 11-year single centre
experience. Eur J Surg Oncol. Jun 2013;39(6):548-53
2. Bailey and Love edition 26th page 1116
3. Robins and cotrans pathologic basis of disease 7th edition
4. [Best Evidence] Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a
systematic review and meta-analysis of prospective observational studies. Lancet. Feb 16
2008;371(9612):569-78.
5. Tumors of the gallbladder. In: Blumgart LH, ed. Surgery of the Liver, Biliary Tract, and Pancreas. 4th ed.
Philadelphia, Pa: Saunders Elsevier; 2007:764-81
6. American Joint Committee on Cancer. Gallbladder. In: AJCC Cancer Staging Manual. 6th ed. New York,
NY: Springer; 2002:139-44.
7. Zielinski MD, Atwell TD, Davis PW, et al. Comparison of surgically resected polypoid lesions of the
gallbladder to their pre-operative ultrasound characteristics. J Gastrointest Surg. Jan 2009;13(1):19-25.
8. [Best Evidence] Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a
systematic review and meta-analysis of prospective observational studies. Lancet. Feb 16
2008;371(9612):569-78.
9. Duffy A, Capanu M, Abou-Alfa GK, et al. Gallbladder cancer (GBC): 10-year experience at Memorial
Sloan-Kettering Cancer Centre (MSKCC). J Surg Oncol. Dec 1 2008;98(7):485-9.
10. NCCN Clinical Practice Guidelines in Oncology™. Available at www.nccn.org.
11. Okada K, Kijima H, Imaizumi T, et al. Wall-invasion pattern correlates with survival of patients with
gallbladder adenocarcinoma. Anticancer Res. Feb 2009;29(2):685-91.
12. 10. Zarin M, Ahmed M, Gohar A, Waheed D, Khurram S, Aurangzeb M, et al. Incidence of Gall stones in
carcinoma gallbladder patients. Pak J Surg 2005;21(1):19-22.](https://image.slidesharecdn.com/gallbladdercarcinoma-141118064126-conversion-gate01/85/Gall-Bladder-Carcinoma-40-320.jpg)


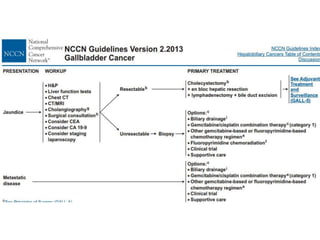
The document details a case summary of a 40-year-old female diagnosed with poorly differentiated adenocarcinoma of the gallbladder, initially presenting with abdominal pain and gallstones, followed by imaging that revealed lymph node involvement. It discusses gallbladder cancer as a malignant disease, its epidemiology, diagnostic workup, potential therapies, and staging based on the TNM classification. The prognosis varies significantly depending on cancer stage, with early-stage detection linked to higher survival rates.























































































