Downloaded 64 times
![PANCREATIC NEOPLASMS
-Dr.Anusha
Moderator: Dr.B.Mohan Lal Naik
M.S[Professor]
Dr.Malleswari M.S[Asst]
Dr.Madhava Krishna M.S [Asst]](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-1-320.jpg)
![ CLASSIFICATION:
Exocrine Tumours:
-Benign :Benign Cystadenomas
-Malignant :Adenocarcinoma[Ampulla/head]
Cystadenocarcinoma
Endocrine Tumours:
-Insulinomas
-Gastrinomas
-Glucaganomas
-VIPomas](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-2-320.jpg)
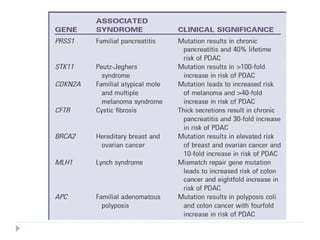
![ Familial Adenomatous Polyposis (FAP) :
APC Gene [Adenomatous Polyposis coli]
Individuals affected by familial adenomatous
polyposis are also significantly more likely to develop
pancreatic cancer.
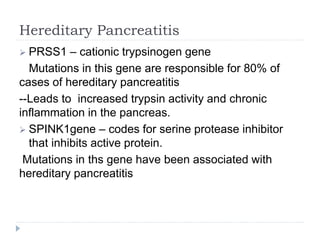
Familial pancreatitis:
Unknown genetic mutations.
-Defined by families with two or more first degree
relatives wih pancreatic ductal adenocarcinoma that
do not fulfill the criteria of other inherited tumour
syndromes with an increased risk for development of
PDAC.](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-13-320.jpg)
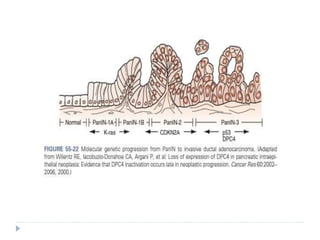
![Sporadic Pancreatic Cancer:
--Most cases are sporadic.
--Development of PDAC from Pancreatic intraepithelial
Neoplasia [PanIn].
--Multiple Tumour suppressor genes and oncogenes
have been identified that play a sigificant role in the
pathogenesis of PDAC
PDX1, KRAS2, CDKN2A, P53 and DPC4/SMAD4.](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-14-320.jpg)
![ KRAS2 Oncogene:
--Mutation of KRAS2 oncogene is one of the earliest
genetic abnormalities identified in progression of PanIn
to PDAC.
--Activated in more than 95% of pancreatic cancers
and is thought to be the initiating event in
tumourigenesis.
--KRAS2 is activated by point mutation [codon 12, 13,
61] , which causes constitutive activation and loss of
regulation of mitogen activated protein kinase cell
signal transduction.](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-15-320.jpg)
![ New onset Diabetes in an elderly patient with weight
loss may be an early presenting symptom of
pancreatic cancer.
Left supraclavicular lymphnode enlargement
Secondaries in Rectovesical pouch [Blumer Shelf]
Periumbilical Lymphadenopathy [Sister Mary Joseph
Nodules]
Gallbladder may be palpable, nontender, moving
with respiration.
Liver enlargement– Secondaries
Ascites](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-22-320.jpg)
![Investigations:
Routine Surgical Profile
Liver Function Tests:
1]Serum bilirubin – Direct component increased
2]Serum Albumin – Decreased with altered A:G ratio.
3]Prothrombin time is increased.
4]Serum Alkaline Phosphatase is increased](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-23-320.jpg)
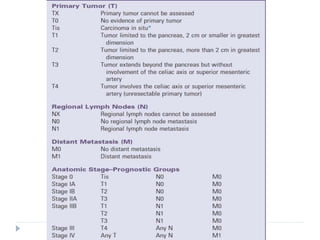
![STAGING :
Based on American Joint Committee on Cancer
tumour, Node, Metstasis [TNM ] system.
Accomplished typically based on Endoscopic
ultrasound guided FNAC, accurately by multidetector
CT scanning of the abdomen and pelvis with three
phase administration of contrast material and three
dimensional reconstruction.](https://image.slidesharecdn.com/carcinomapancreas-180827140005/85/Carcinoma-pancreas-26-320.jpg)


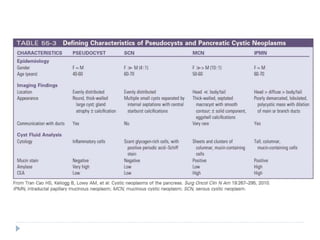


1) The document discusses pancreatic neoplasms, including classification into exocrine and endocrine tumors. 2) It highlights adenocarcinoma of the pancreas, noting risk factors like smoking, chronic pancreatitis, genetics, and more. 3) Diagnosis involves imaging like CT/MRI, blood tests, and pathology examination of biopsies showing malignant cells and fibrosis.




































![Ca pancreas [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/capancreasautosaved-200627065511-thumbnail.jpg?width=640&height=640&fit=bounds)







































