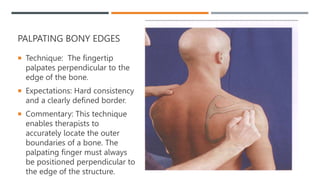
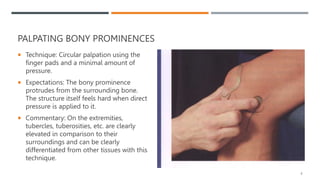
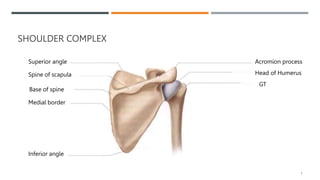
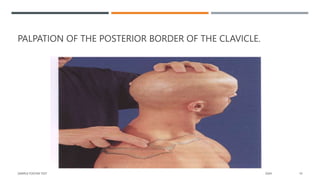
This document provides guidance on palpation techniques for structures in the shoulder complex. It describes how to palpate bony edges and prominences using specific techniques like perpendicular finger placement and circular motions. Key structures of the shoulder girdle that can be palpated are identified, including the scapula, clavicle, and humerus. Reference points and positions are outlined to locate structures and assess shoulder range of motion.































![Shoulder_joint_and_applied_aspects[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shoulderjointandappliedaspects1-240425164911-e75cbd49-thumbnail.jpg?width=640&height=640&fit=bounds)


























![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)






























