Downloaded 92 times


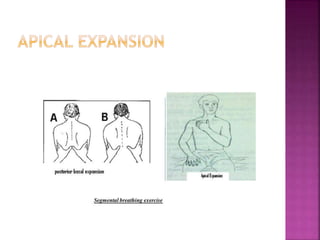


The document discusses breathing exercises and ventilator training for patients with pulmonary diseases or who have undergone surgery. It describes techniques like diaphragmatic breathing, pursed lip breathing, and segmental breathing that aim to improve ventilation, airway clearance, and prevent complications. The types of patients who may benefit are outlined as well as contraindications. Specific instructions for exercises like diaphragmatic breathing and positions are provided.



































































