
More Related Content
What's hot
What's hot (20)
Similar to Manualmusletesting 121 150
Similar to Manualmusletesting 121 150 (20)
Recently uploaded
Recently uploaded (20)
Manualmusletesting 121 150
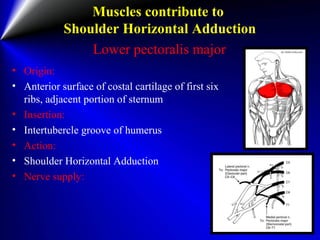
- 1. Muscles contribute to Shoulder Horizontal Adduction Lower pectoralis major • Origin: • Anterior surface of costal cartilage of first six ribs, adjacent portion of sternum • Insertion: • Intertubercle groove of humerus • Action: • Shoulder Horizontal Adduction • Nerve supply:
- 2. Normal & Good • Position: • Supine with arm abducted to 90 degrees. • Stabilization: • Stabilize scapula to prevent abduction of the scapula. • Palpation: • Below and near the origin at sternal end of the clavicle. • Desired Motion: • Patient adducts arm through range of motion. • Resistance: • Is given proximal to elbow joint. Palpation
- 3. Fair • Position: • Supine with arm abducted to 90º. • Stabilization: • Stabilize scapula to prevent abduction of the scapula. • Palpation: • Below and near the origin at sternal end of the clavicle. • Desired motion: • Patient adducts arm to vertical position.
- 4. Poor • Position: • Sitting with arm resting on table in 90º of abduction. • Stabilization: • Stabilize trunk. • Palpation: • Below and near the origin at sternal end of the clavicle. • Desired motion: • Patient brings arm forward through ROM.
- 5. Trace & Zero • Examiner palpates tendon of Pectoralis major near insertion on anterior aspect of upper arm. • Muscle fibers of both sternal and clavicular portions may be observed and palpated on upper anterior aspect of thoracic.
- 6. Note • Factor limiting Motion: • Tension of shoulder extensor muscles • Contact of arm with trunk. • Fixation: • In forceful horizontal adduction, contraction of Obliquus externus abdominus muscle on same side. • Substitution: • 1-Anterior portion of deltoid • 2-Coracobrachialis • 3- Short Head of biceps.
- 7. Shoulder External Rotation Teres Minor Infraspinatus
- 8. Muscles contribute to Shoulder External Rotation Teres Minor • Origin: • Posteriorly on upper & middle aspect of lateral border of scapula • Insertion: • Posterior surface of greater tubercle of the humerus • Action: Shoulder Extension • Nerve supply:
- 9. Muscles contribute to Shoulder External Rotation Infraspinatus • Origin: • Posteriorly on upper & middle aspect of lateral border of scapula • Insertion: • Posterior surface of greater tubercle of the humerus • Action: Shoulder Extension • Nerve supply:
- 10. Normal & Good • Position: • Prone with shoulder abducted to 90º, upper arm supported on table and lower arm hanging vertically over edge. • Stabilization: • Stabilize scapula with hand and forearm, but allow freedom for rotation. • Palpation point: • None • Desired motion: • Patient swings lower arm forward and up-ward and 'laterally rotates shoulder through range of motion. • Resistance: • Is given above wrist on forearm.
- 11. Fair • Position: • Prone with shoulder abducted to 90º, upper arm supported on table and lower arm hanging vertically over edge. • Stabilization: • Stabilize scapula and place hand against anterior surface of arm to prevent abduction (without interfering with motion). • Palpation: • None • Desired motion: • Patient swings lower arm forward and up-ward and laterally rotates shoulder through ROM.
- 12. Poor • Position: • Prone with entire arm over edge table in medially rotated positron. • Stabilization: • Stabilize scapula. • Palpation: • None • Desired Motion: • Patient laterally rotates arm through range of motion. (supination of the forearm should not be allowed to substitute for full range in lateral rotation.)
- 13. Trace & Zero • The Teres minor may be palpated on axillary border of scapula, and Infraspinatus over body of scapula below the spine.
- 14. Note • Factors Limiting Motion: • a- Tension of superior portion of scapular ligament. • b- Tension of lateral rotator muscles of shoulder. • Fixation: • a- Weight of trunk. • b- Contraction of Trapezius and Rhomboid major and minor muscles to fix scapula • Substitutions: 1. Wrist extensors 2. Roll the shoulder backwards.
- 15. Shoulder Internal Rotation Subscapularis U. Pectoralis Major Latissimus DorsiL. Pectoralis Major
- 16. Muscles contribute to Shoulder Internal Rotation Subscapularis • Origin: • Anterior surface of subscapular fossa • Insertion: • Lesser tubercle of the humerus • Action: • Shoulder Internal Rotation • Nerve supply:
- 17. Muscles contribute to Shoulder Internal Rotation Upper pectoralis major • Origin: • Medial half of anterior surface of clavicle • Insertion: • Intertubercle groove of humerus • Action: • Shoulder Internal Rotation • Nerve supply:
- 18. Muscles contribute to Shoulder Internal Rotation Lower pectoralis major • Origin: • Anterior surface of costal cartilage of first six ribs, adjacent portion of sternum • Insertion: • Intertubercle groove of humerus • Action: • Shoulder Internal Rotation • Nerve supply:
- 19. Muscles contribute to Shoulder Internal Rotation Latissimus dorsi • Origin: • a- Spines of lower 6 thoracic and lumbar vertebrae • b- Posterior surface of sacrum& Posterior aspect of crest of ileum • c- Lower 3-4 ribs • d- Inferior angle of scapula • Insertion: • Intertubercle groove of humerus • Action: • Shoulder Internal Rotation • Nerve supply:
- 20. Normal & Good • Position: • Prone with shoulder abducted to 90 degrees, upper arm supported on table and lower arm hanging vertically over edge. • Stabilization: • Stabilize scapula with hand and forearm, but allow freedom for rotation. • Palpation: • None • Desired Motion: • Patient swings lower arm backward and up- ward and medially rotates shoulder through range of motion. • Resistance: • Is proximal to wrist on forearm.
- 21. Fair • Position: • Prone with shoulder abducted to 90 degrees, upper arm supported on table and lower arm hanging vertically over edge. • Stabilization: • Stabilize scapula. • Palpation: • None • Desired Motion: • Patient swings lower arm backward and up-ward and medially rotates shoulder through range of motion.
- 22. Poor • Position: • Prone with arm over edge of table in lateral rotation. • Stabilization: • Stabilize scapula. • Palpation: • None • Desired Motion: • Patient medially rotates arm through range of motion. (Pronation of the forearm should not be allowed to substitute for full range in medial rotation.)
- 23. Trace & Zero • Fibers of Subscapularis may be palpated deep in axilla near insertion.
- 24. Shoulder Abduction to 90º Middle Deltoid Supraspinatus
- 25. Muscles contribute to Shoulder Abduction to 90º Middle Deltoid • Origin: • Acromion process • Insertion: • Deltoid tuberosity on the lateral humerus • Action: • Shoulder Abduction to 90º • Nerve supply:
- 26. Muscles contribute to Shoulder Abduction to 90º Supraspinatus • Origin: • Supraspinatus fossa • Insertion: • Greater tubercle of the humerus • Action: • Shoulder Abduction to 90º • Nerve supply:
- 27. Note • Factors Limiting Motion: • None: range of motion incomplete. • Fixation: • Contraction of Trapezius and Serratus anterior muscles. • Serratus anterior and upper fibers of trapezius assist in upward rotation of scapula as well as in fixation.
- 28. Normal & Good • Position: • Sitting with arm at side in mid-position between medial and lateral rotation. • Elbow flexed a few decrees. • Stabilization: • Stabilize scapula. • Palpation: • Just below the acromion process of the scapula. • Desired Motion: • Patient abducts the humerus to 90º(palm down). • Resistance : • Is given proximal to elbow
- 29. Fair • Position: • Sitting with arm at side in midposition between medial and lateral rotation. • Elbow flexed a few degrees. • Stabilization: • Stabilize scapula. • Palpation: • Just below the acromion process. • Desired Motion: • Patient abducts arm to 90º (palm down).
- 30. Poor • Position: • Supine with arm at side in midposition between medial and lateral rotation. • Elbow slightly flexed. • Stabilization: • Stabilize scapula over acromion. • Desired Motion: • Patient abducts arm to 90º without Lateral rotation at shoulder joint Alternate