Downloaded 388 times
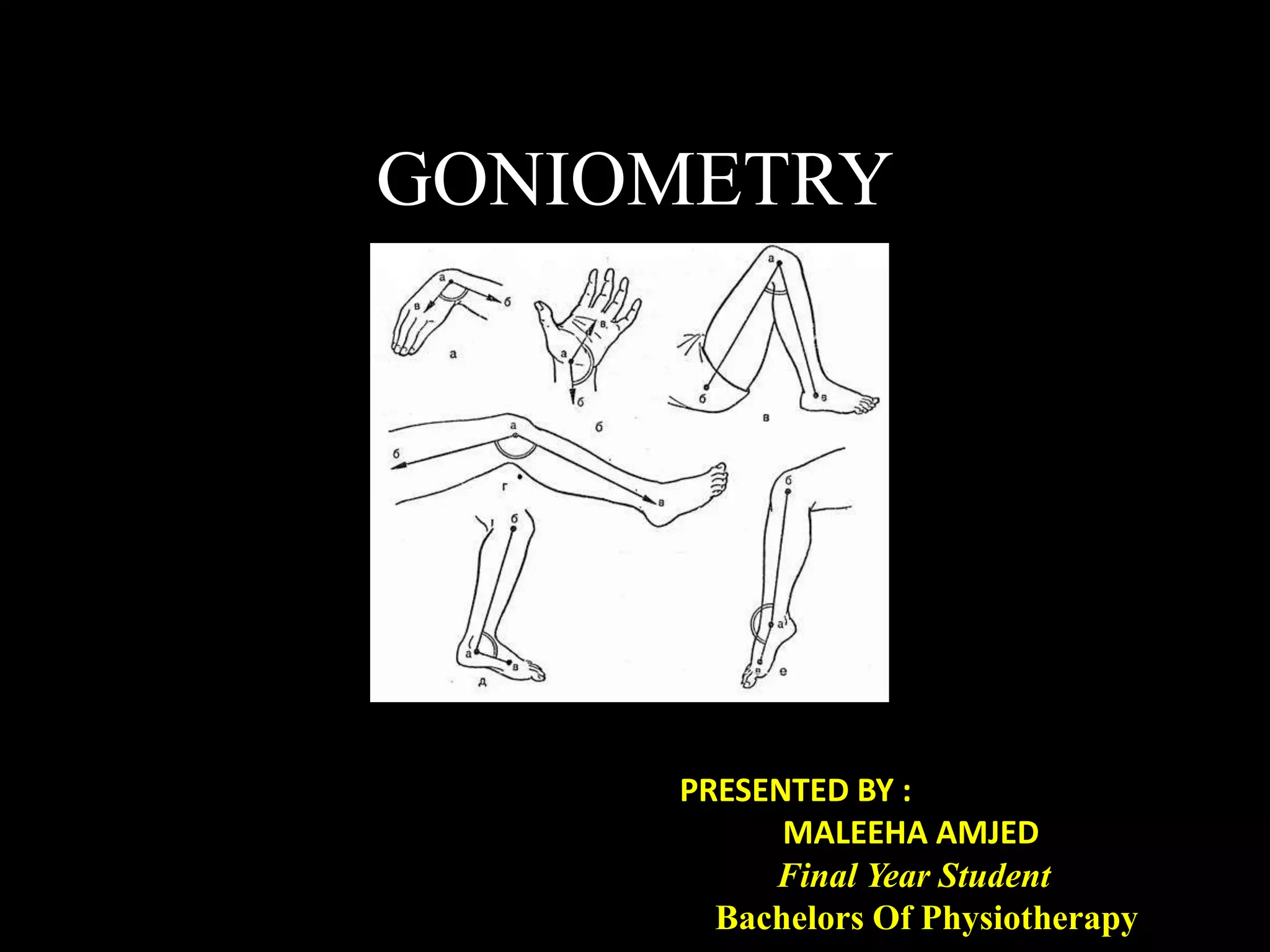
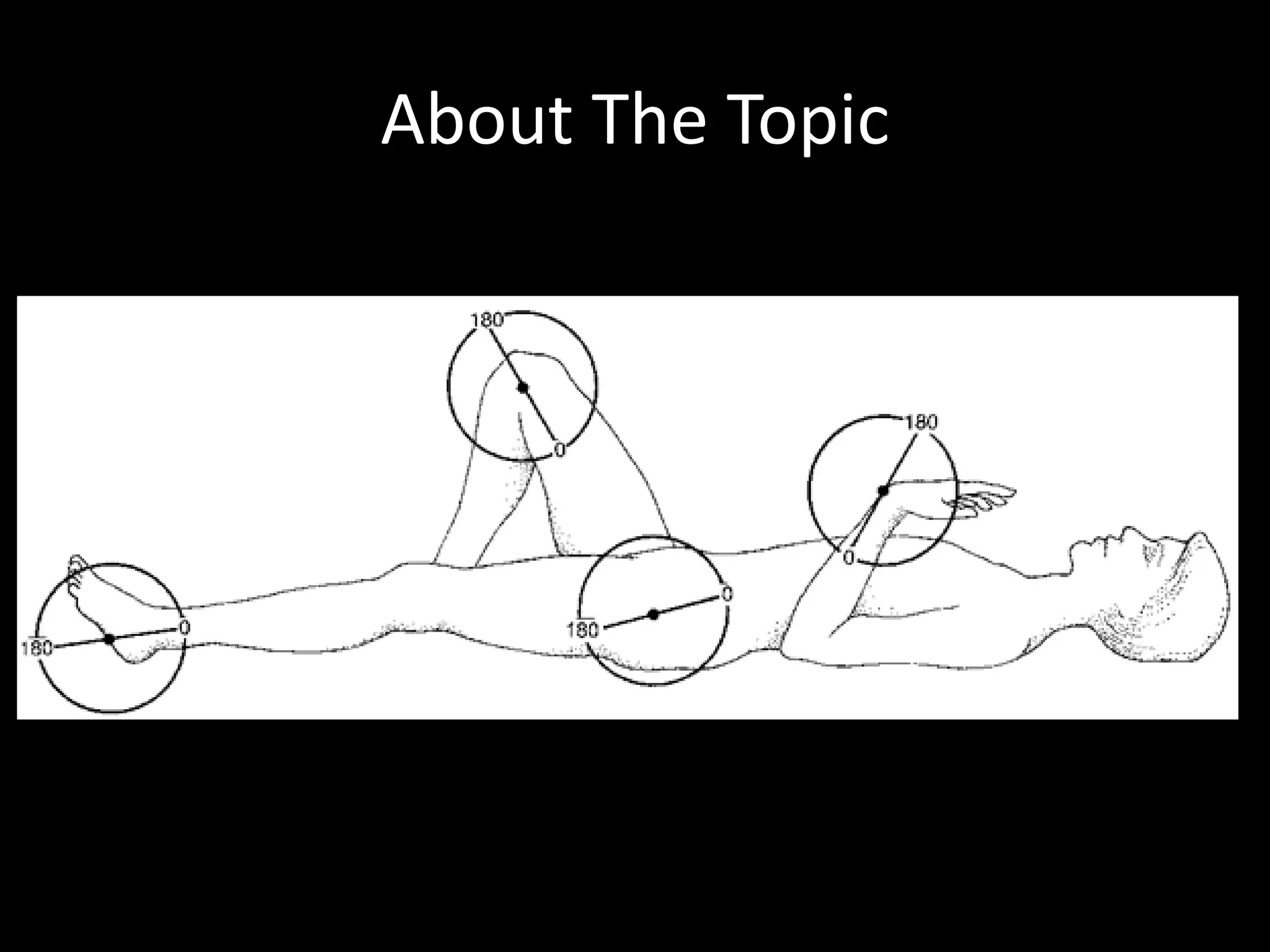









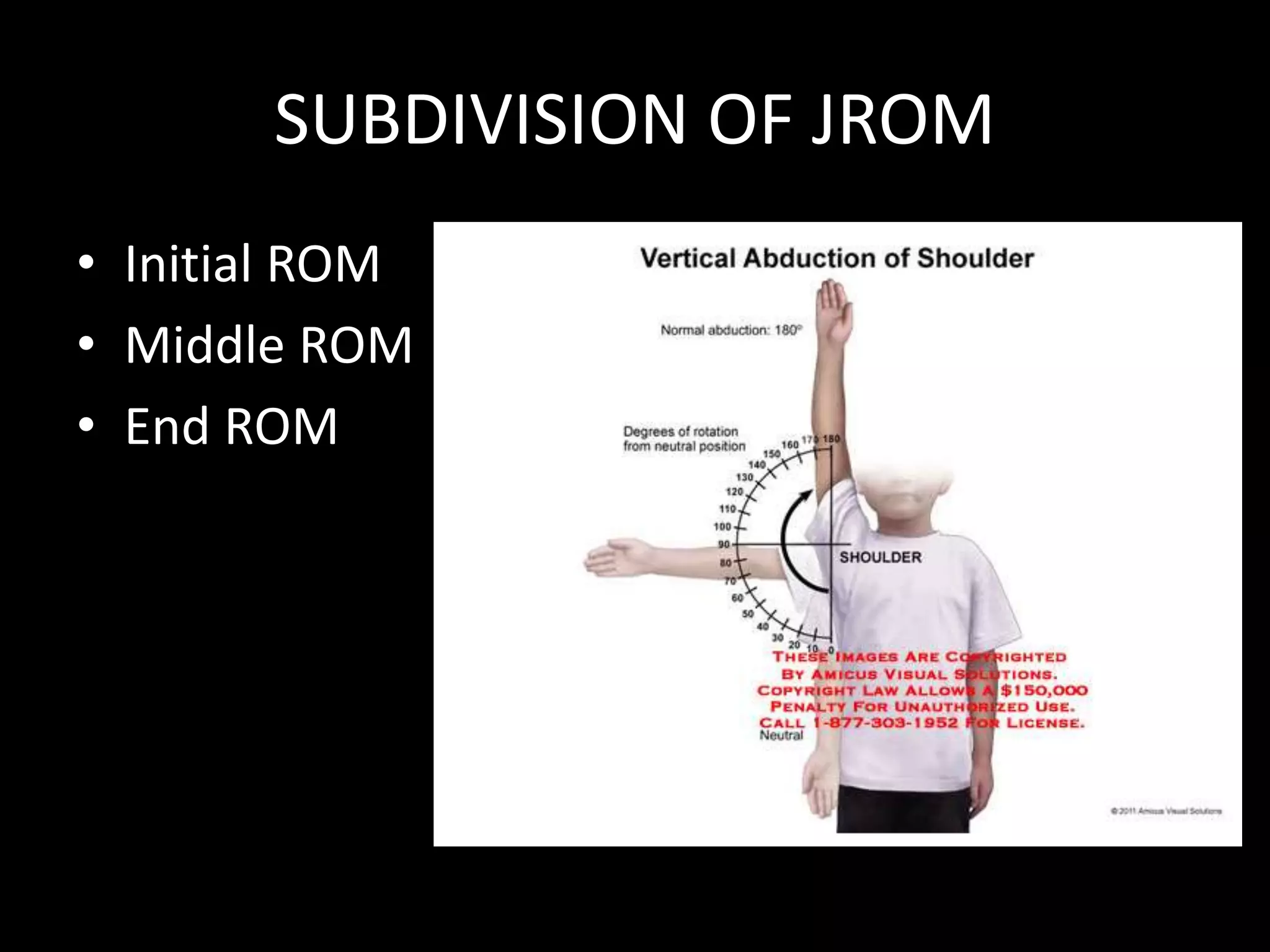














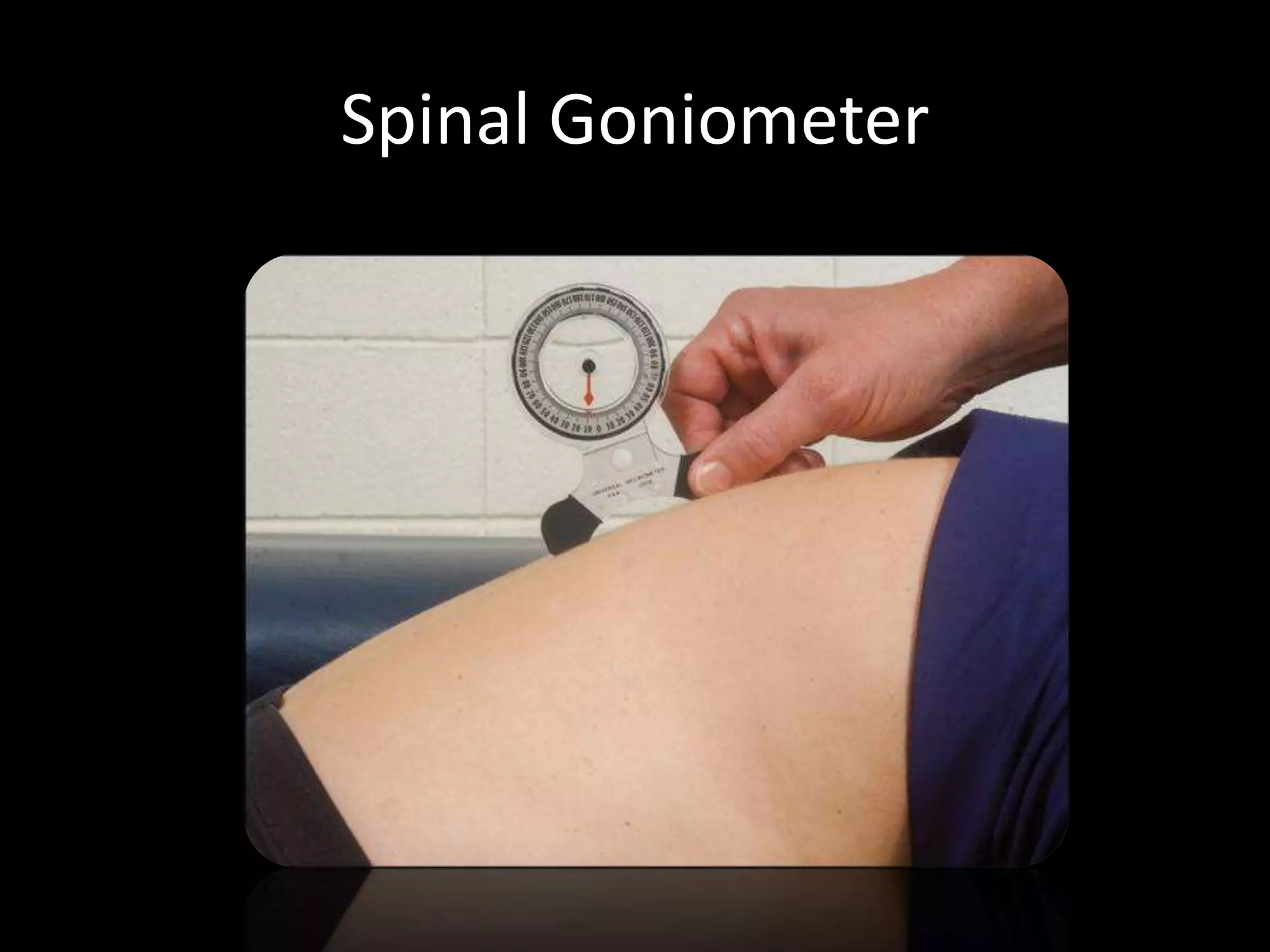
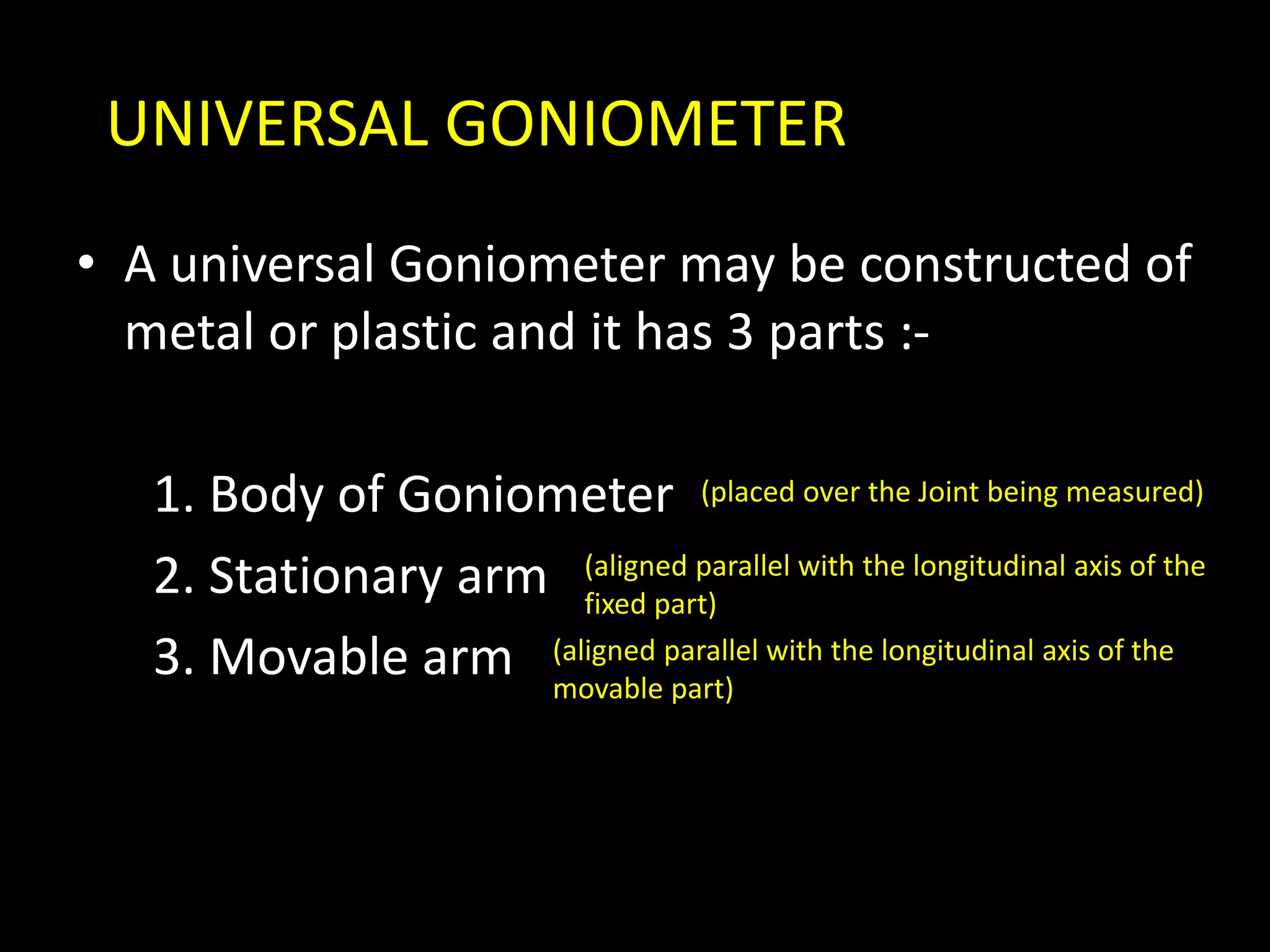





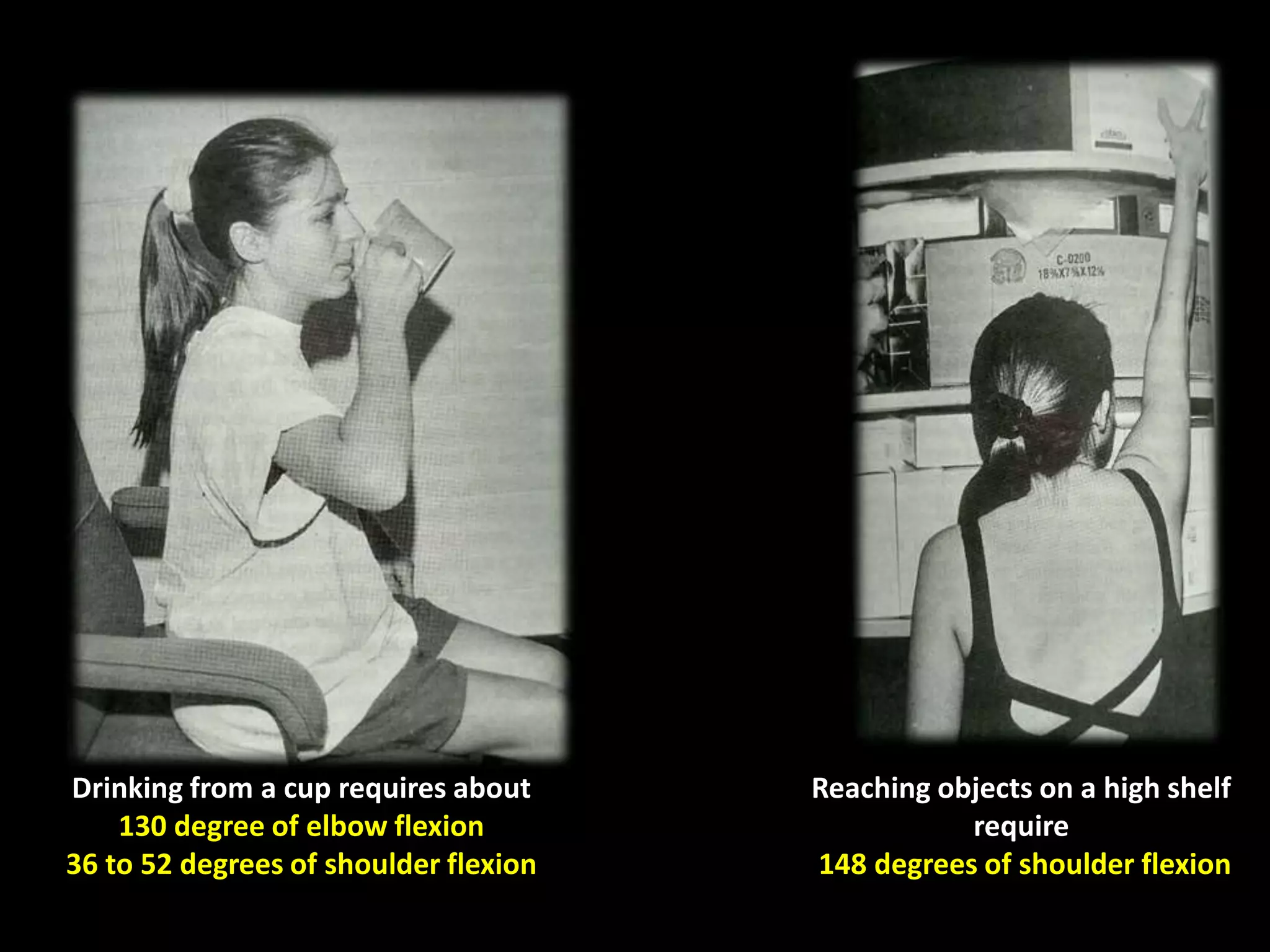











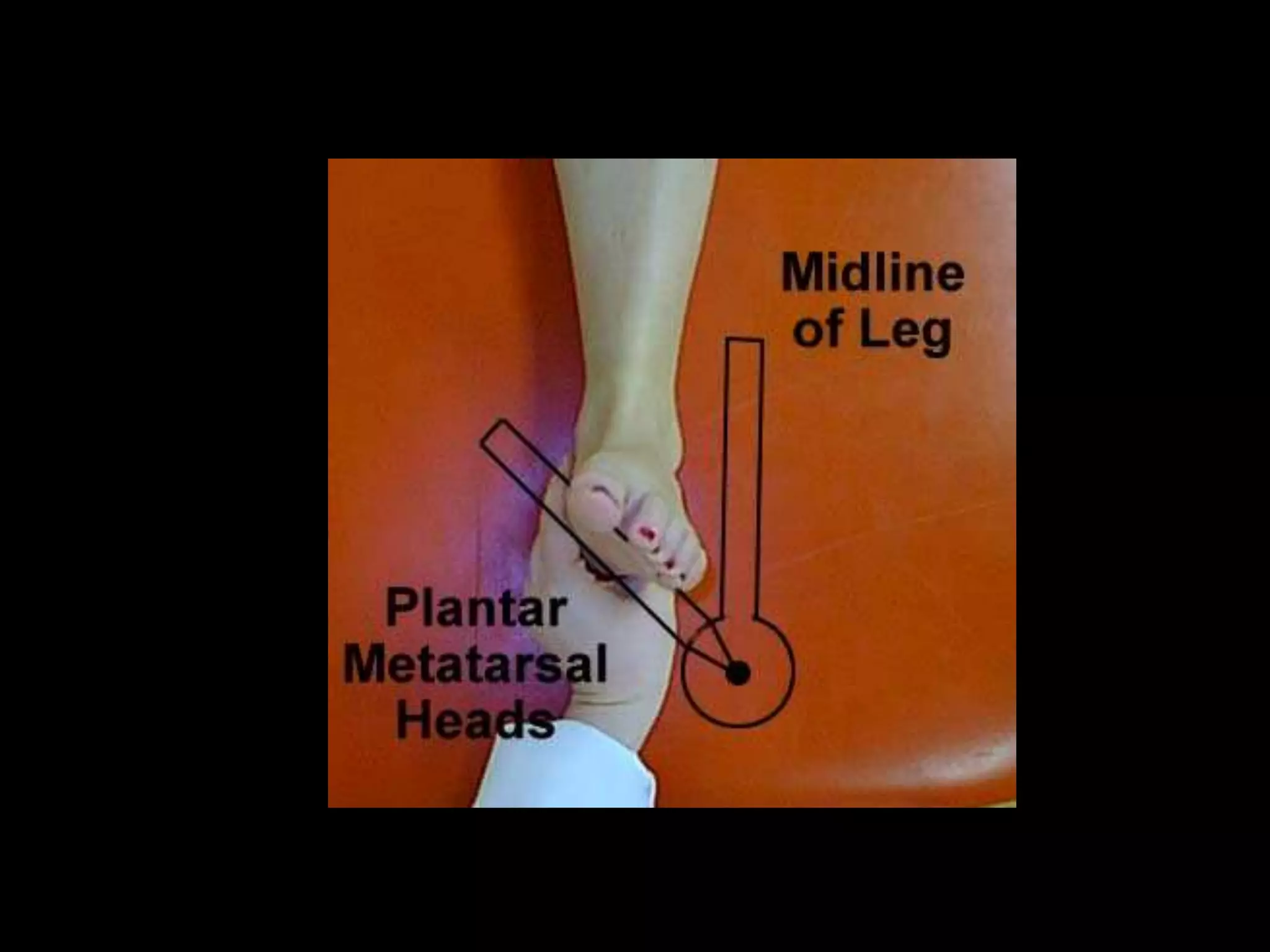

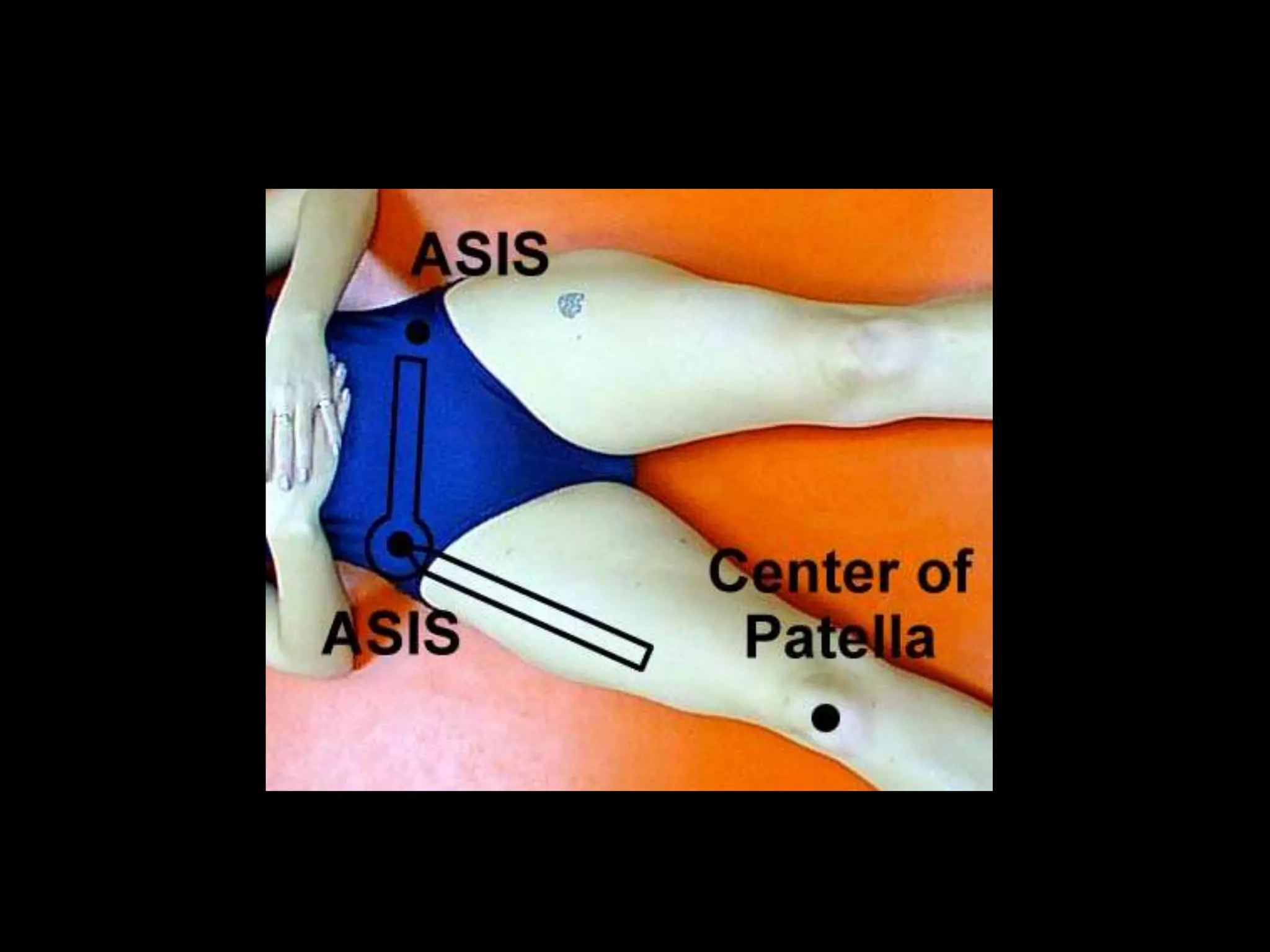


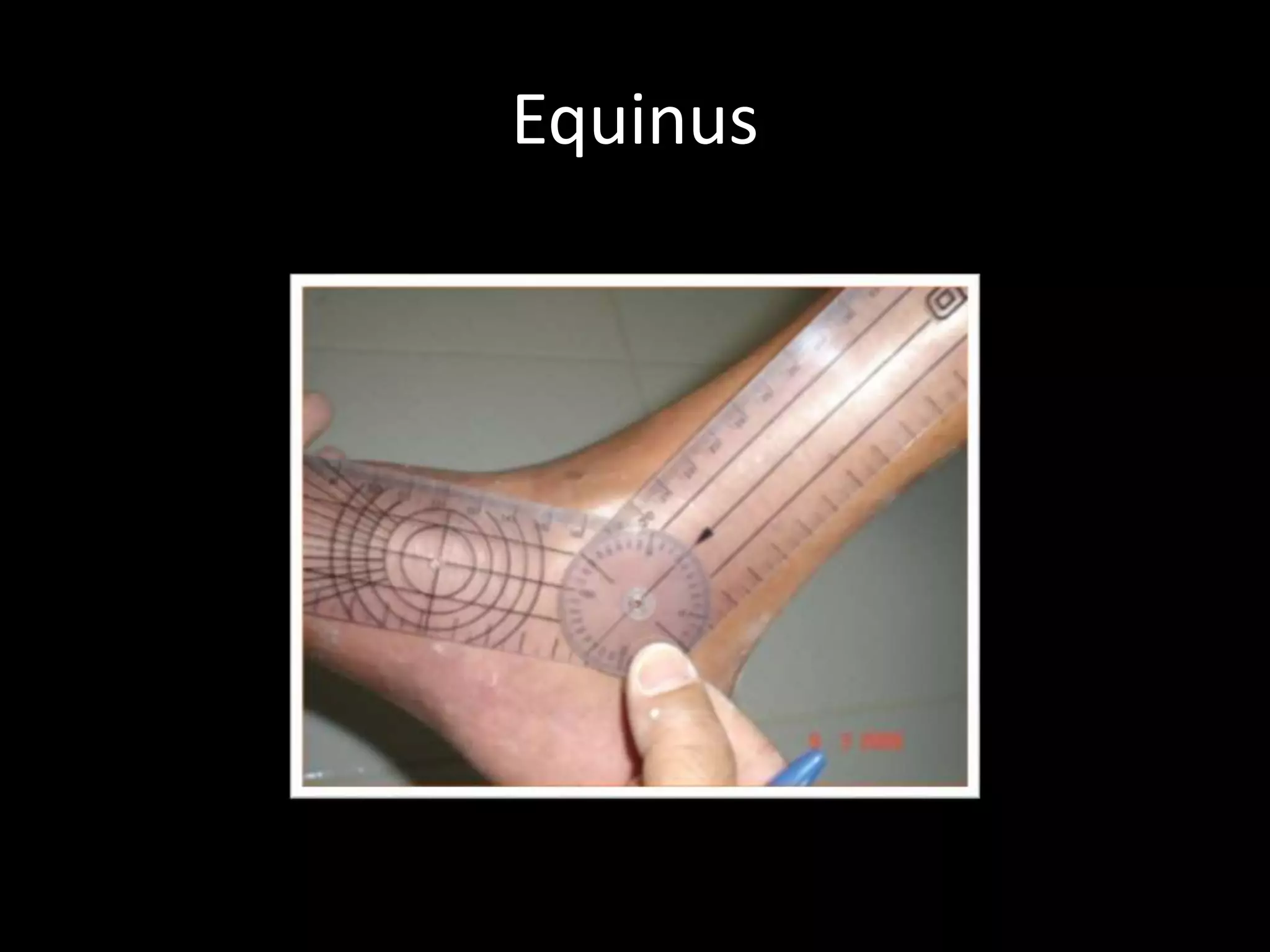

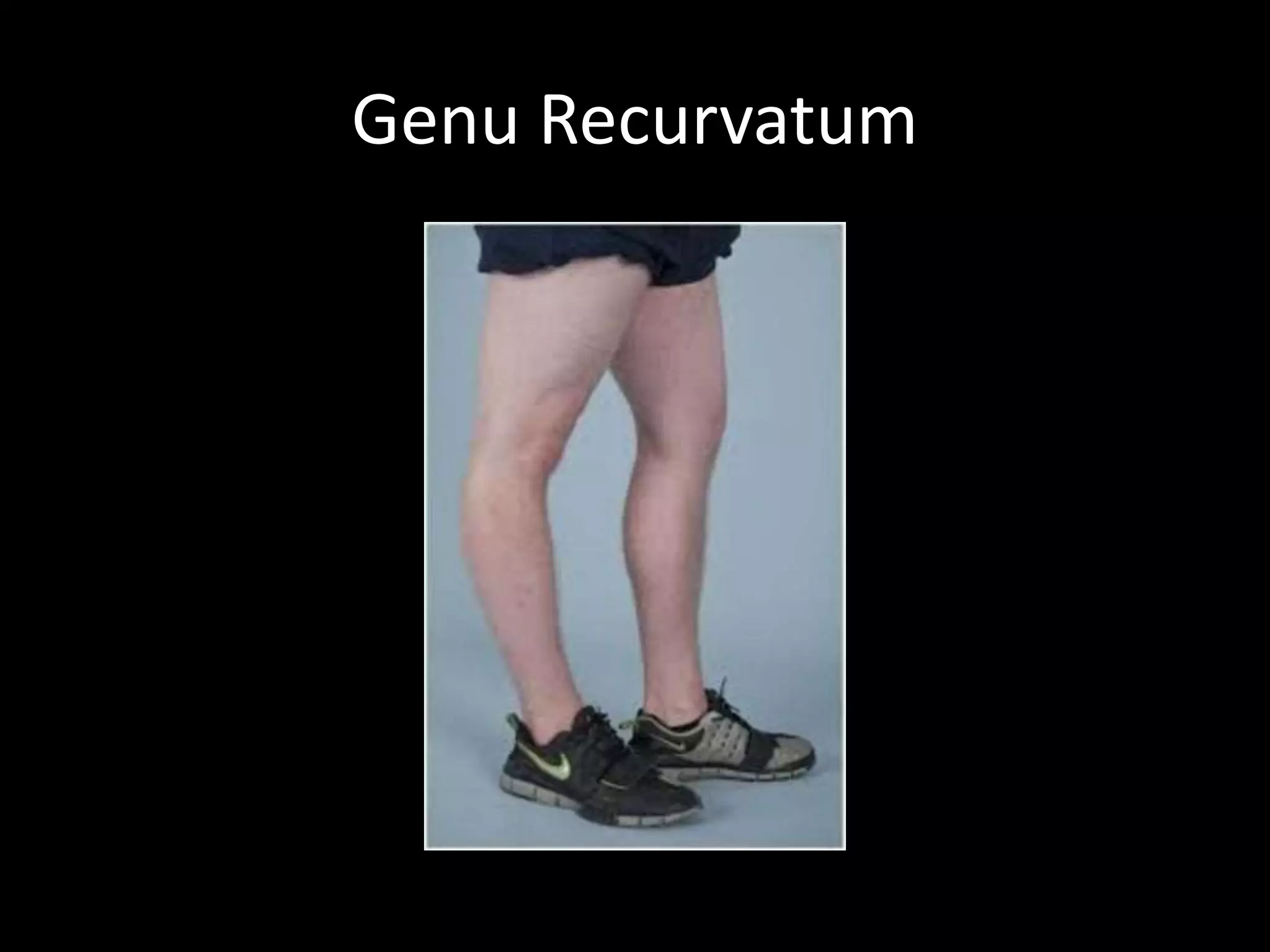



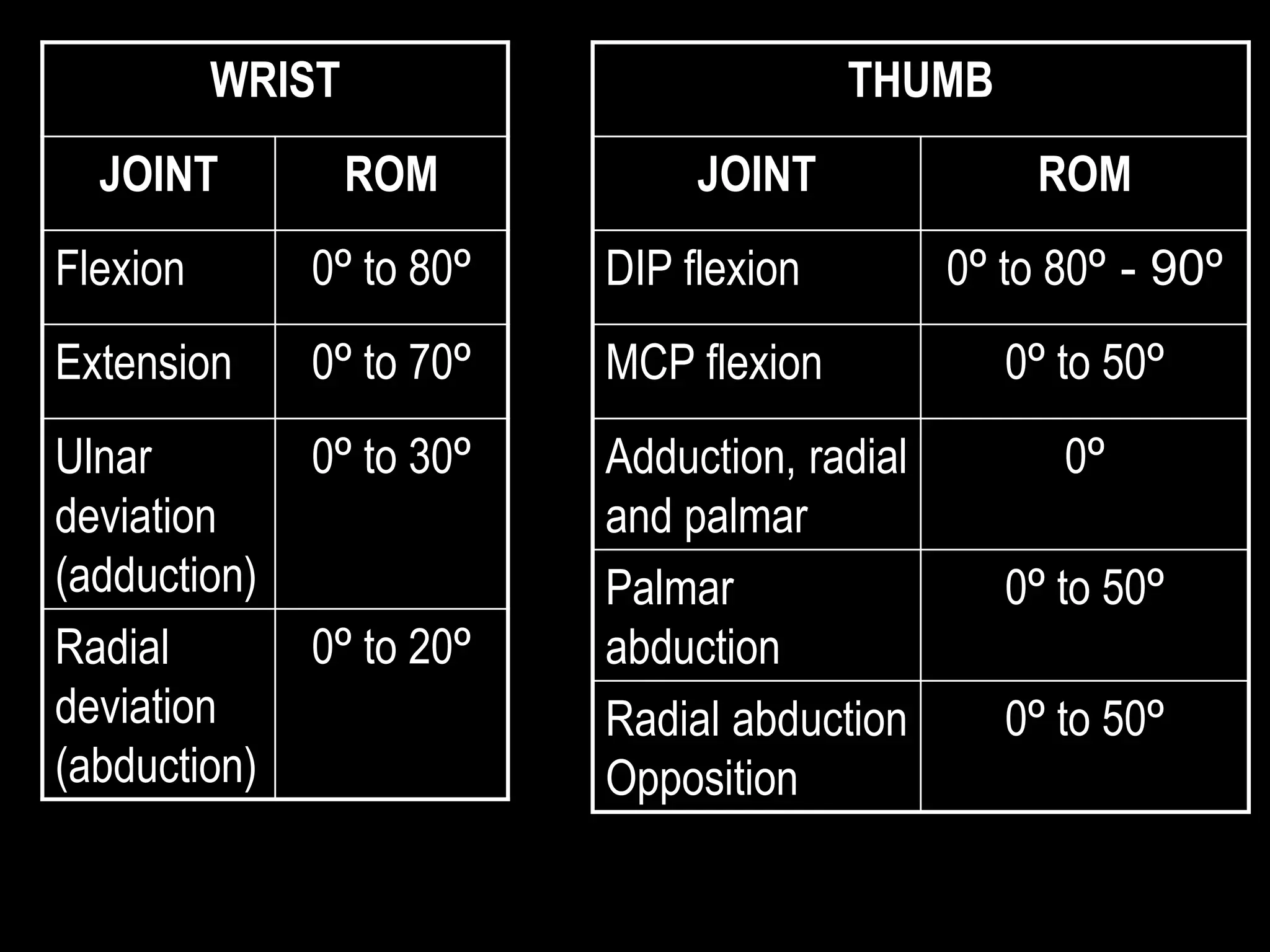

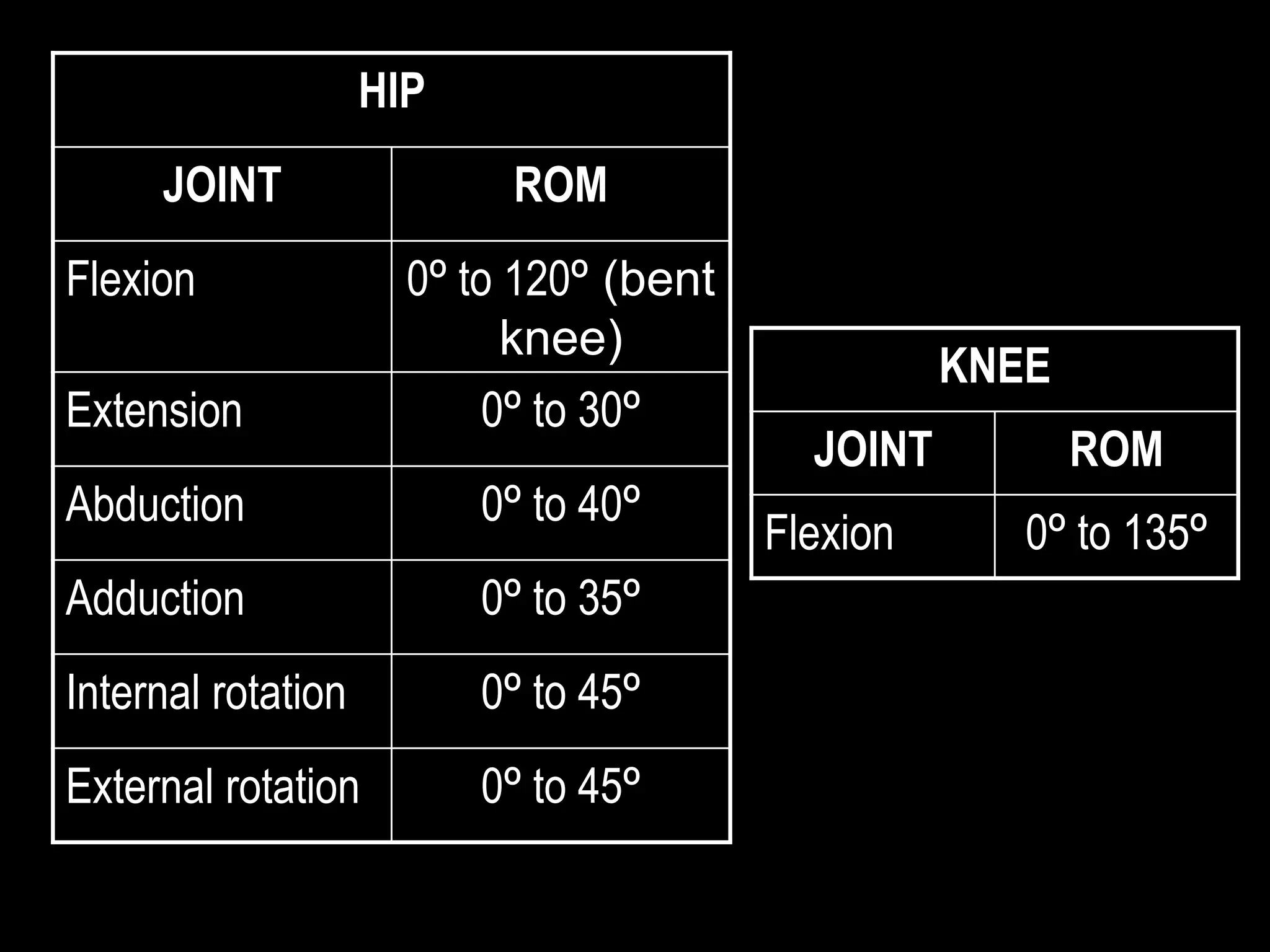


Goniometry refers to the measurement of joint angles in the human body. It is an important part of a physical examination to determine range of motion, evaluate progress, and modify treatment. There are different types of goniometers used to measure motion in various planes at joints like the shoulder, elbow, wrist, fingers, hip, and spine. Factors like a person's age, joint health, surrounding soft tissues, and pathological conditions can impact the normal range of motion values. Proper positioning, stabilization, and identification of bony landmarks is required to accurately measure and document a joint's range of motion.



































































