Downloaded 68 times
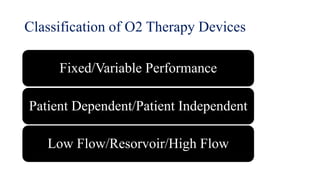
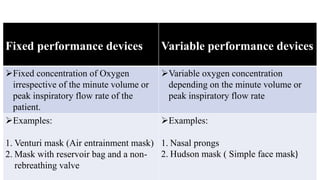


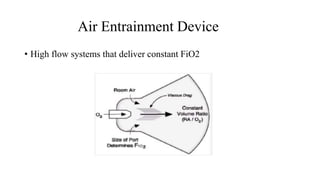

This document discusses various oxygen therapy devices: 1. It classifies devices as fixed or variable performance, patient dependent or independent, and low, reservoir, or high flow. Nasal prongs and Hudson masks are examples of low flow devices while venturi masks are high flow. 2. Nasal prongs deliver 1-6 L/min of oxygen but allow a large fraction of inspired volume from room air. Hudson masks deliver 5-10 L/min and have a maximum FiO2 of 60%. 3. Reservoir bags attached to masks can increase oxygen concentration delivered. Partial rebreathers allow some exhaled gas to re-enter the bag while non-rebreathers prevent inhaling room























































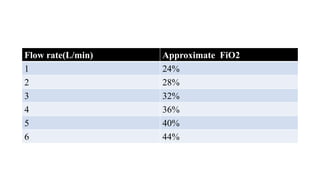
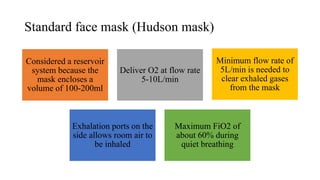
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











