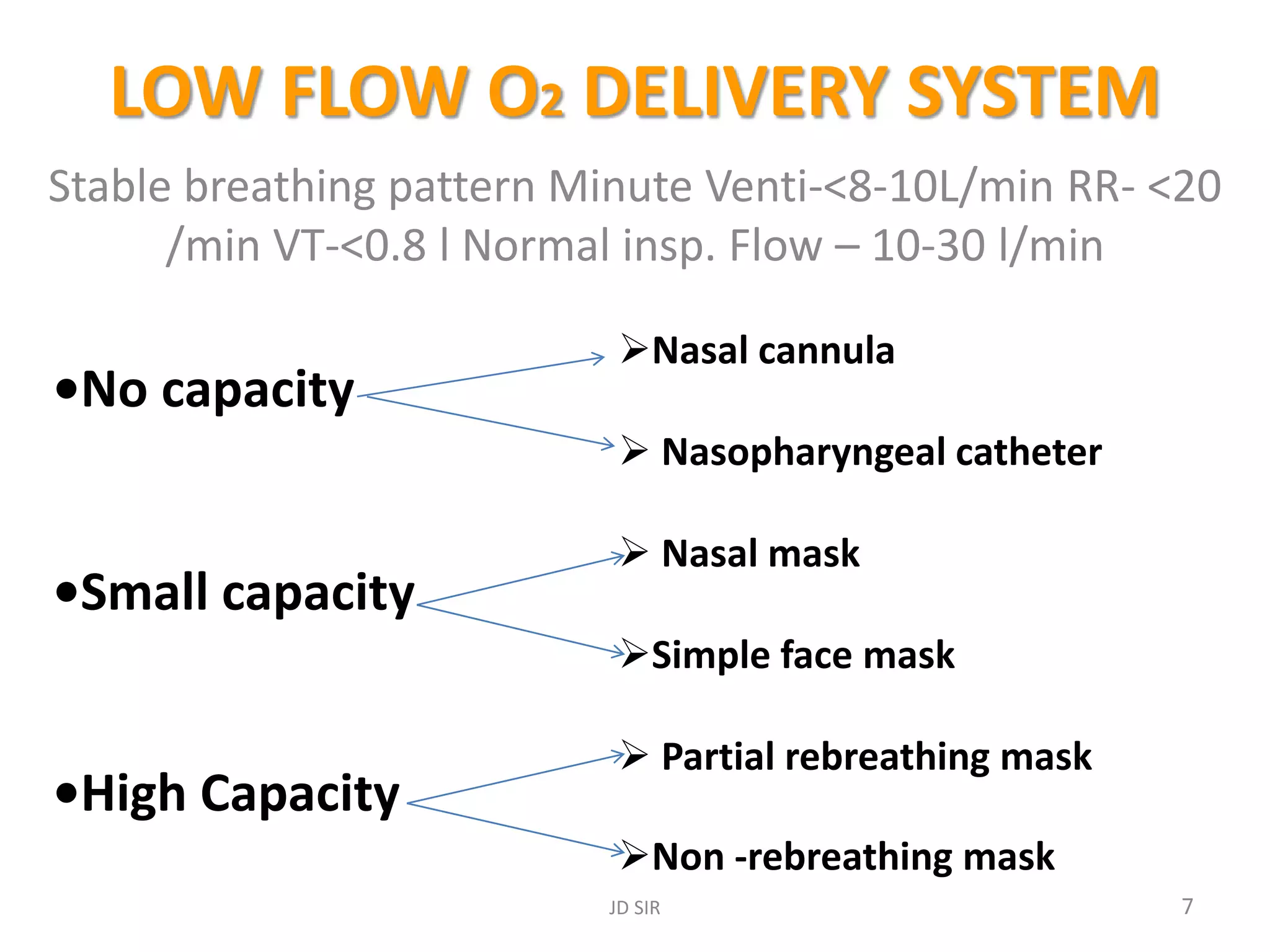
The document discusses oxygen delivery devices and their indications, methods, and complications. It outlines two primary systems: low flow and high flow, detailing various delivery methods such as nasal cannulas, face masks, and Venturi masks, along with their advantages and disadvantages. Additionally, it covers essential clinical goals of oxygen therapy, complications, and safety considerations related to oxygen use.


































































![Oxygen therapy devices [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/oxygentherapydevicesautosaved-170806143146-thumbnail.jpg?width=640&height=640&fit=bounds)






























