Downloaded 1,619 times









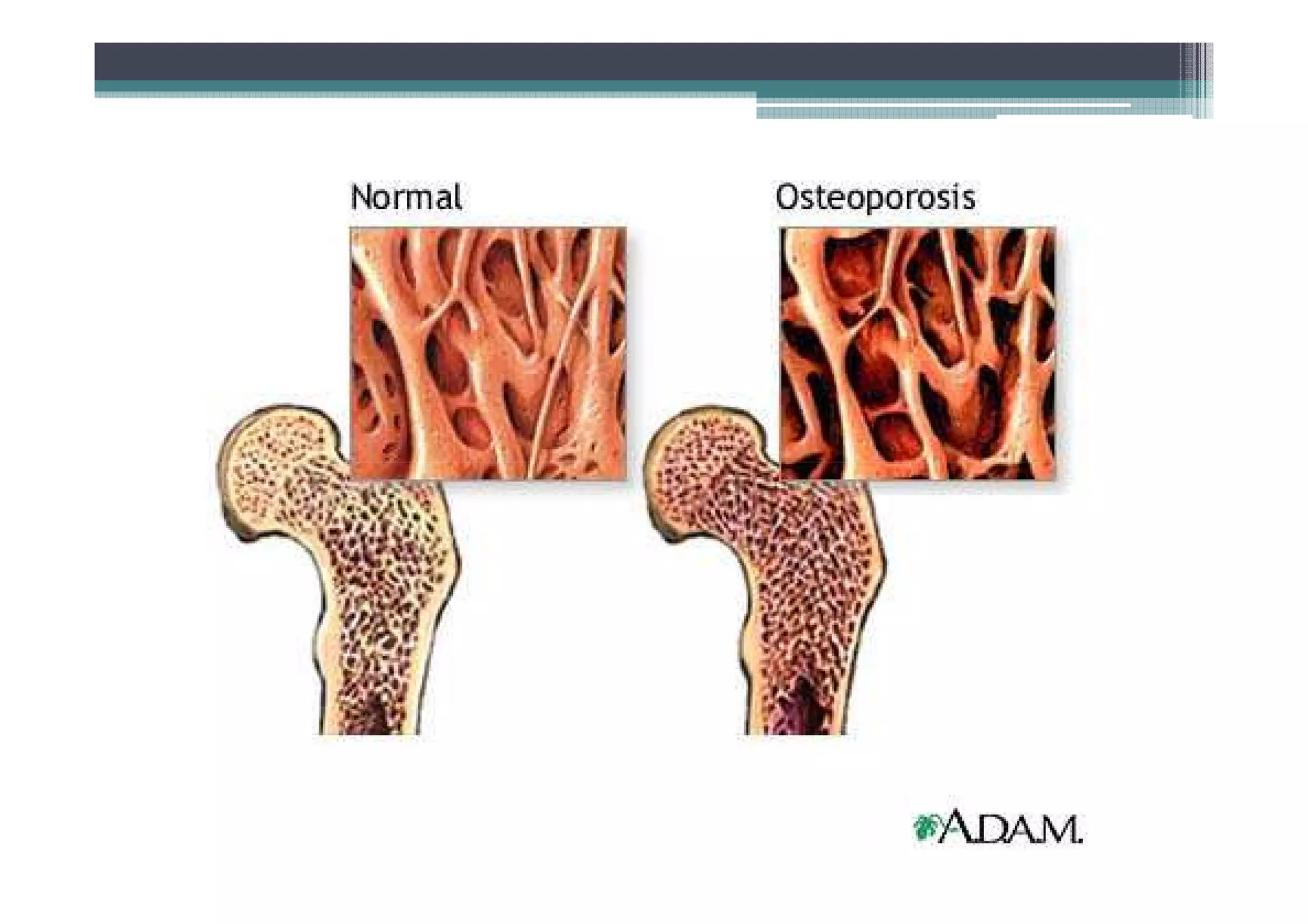






























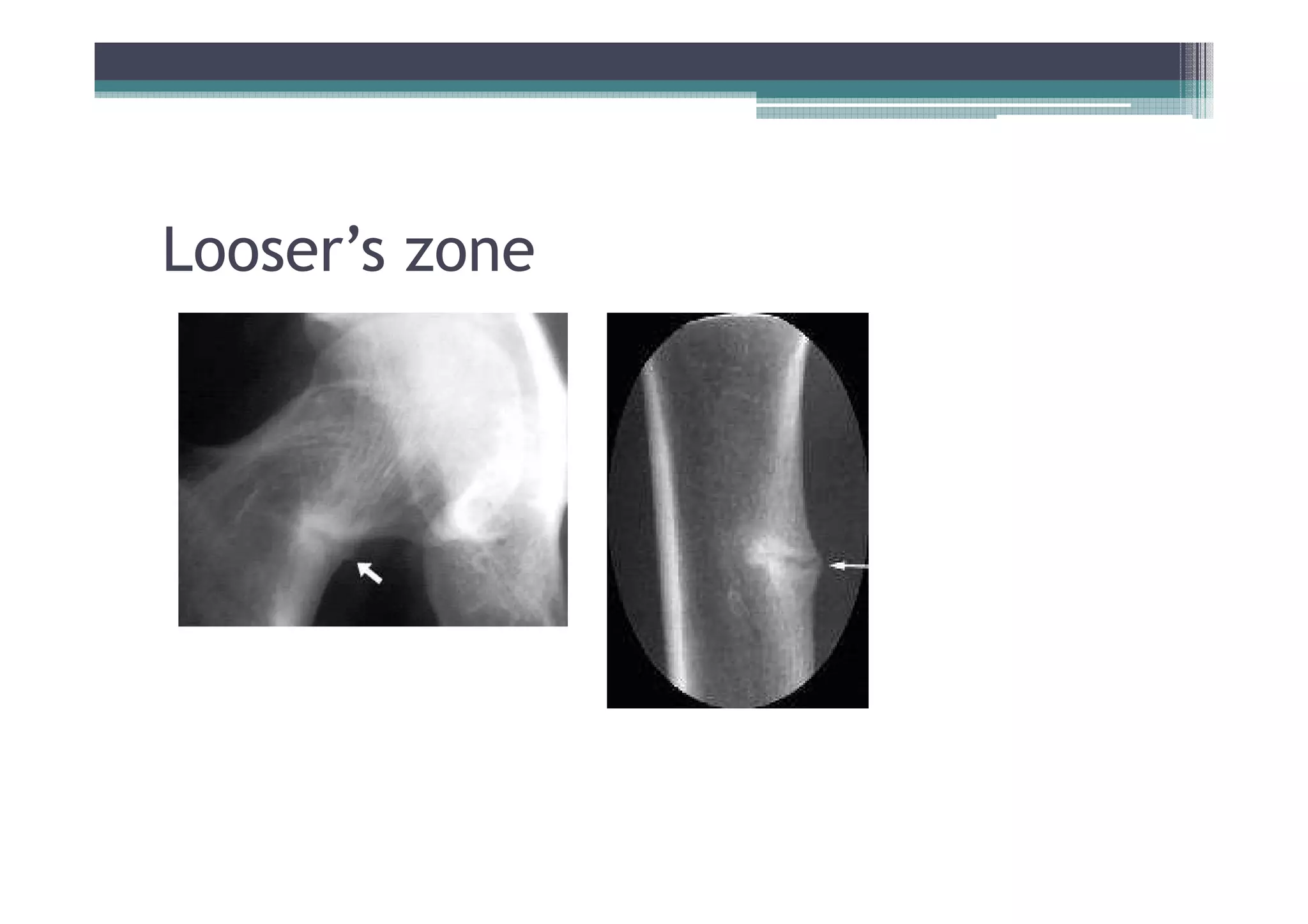












































The document provides an overview of various musculoskeletal disorders, specifically focusing on degenerative and metabolic bone disorders such as osteoporosis, osteomalacia, and Paget’s disease. It outlines risk factors, symptoms, diagnostic methods, and treatment strategies for these conditions, emphasizing the importance of proper vitamin D intake and management approaches. The document also includes specific recommendations for dietary allowances, available treatments, and prognosis for patients affected by these disorders.























































































