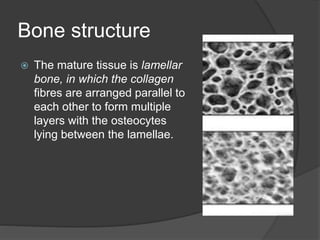
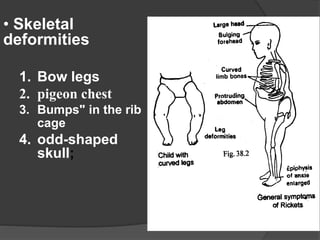
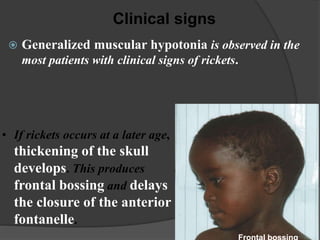
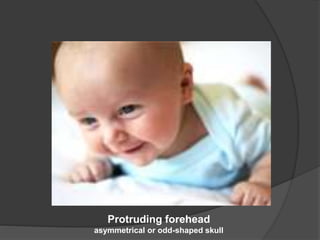
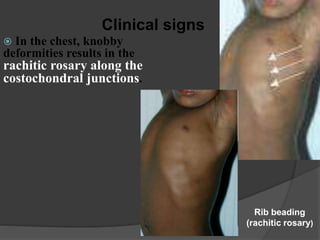
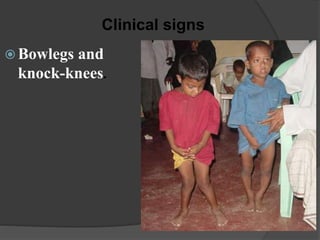
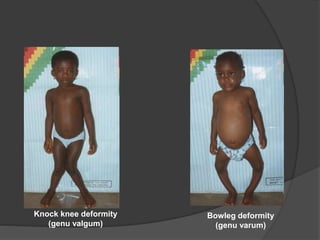
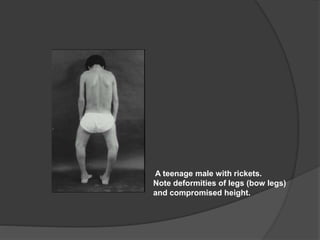
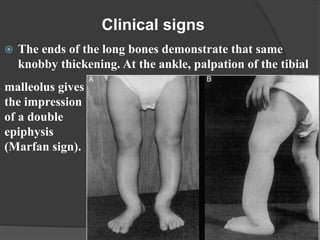
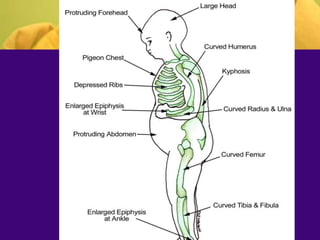
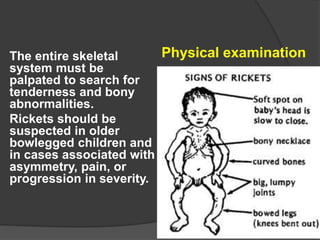
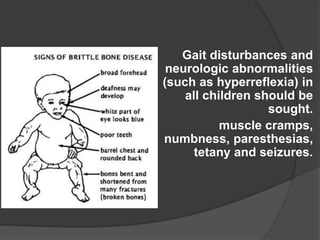
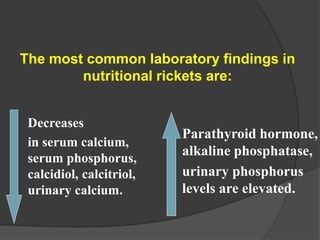
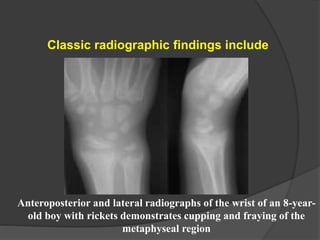
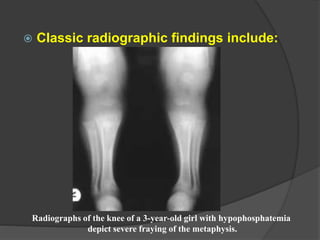
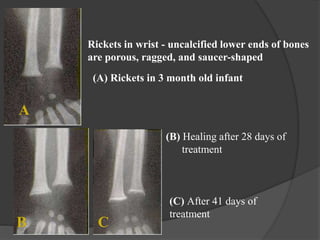
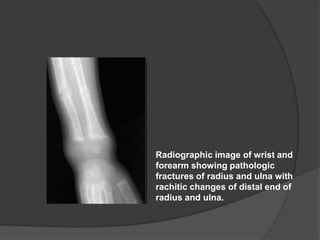
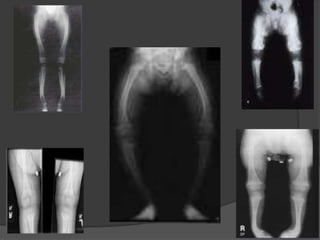
This document discusses rickets, including its causes, signs and symptoms, diagnosis, and treatment. Rickets is caused by a lack of vitamin D, calcium, or phosphate, which can result from inadequate sunlight exposure, poor nutrition, liver or kidney diseases, and some medications. Clinical features include bone deformities, muscle weakness, and growth delays. Diagnosis involves physical exam, lab tests showing low calcium and vitamin D levels and high alkaline phosphatase, and x-rays revealing bone changes. Treatment focuses on high dose vitamin D supplementation in the short term, followed by lower lifelong doses, along with ensuring adequate calcium and phosphate intake.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

