Download to read offline
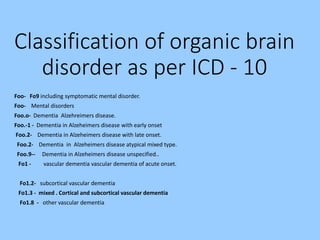
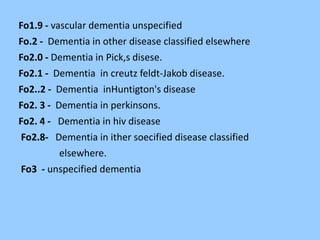
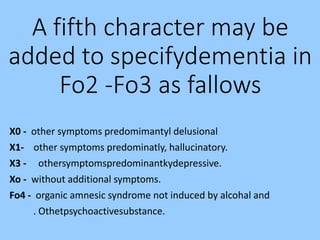
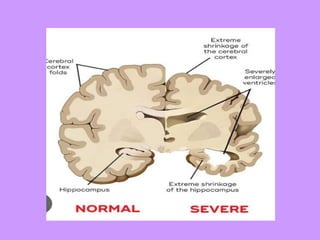

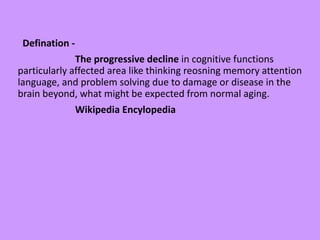
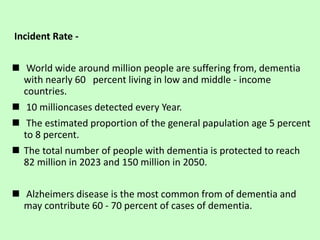
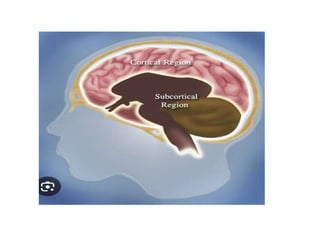

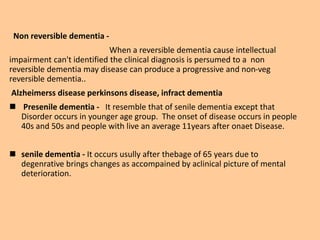
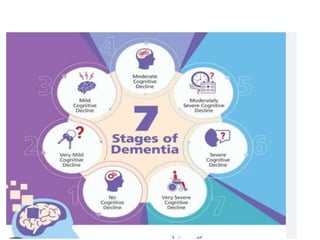
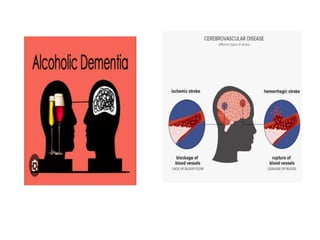
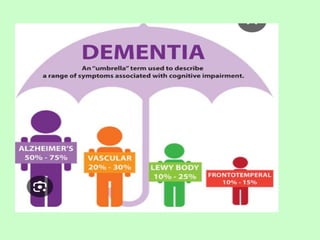
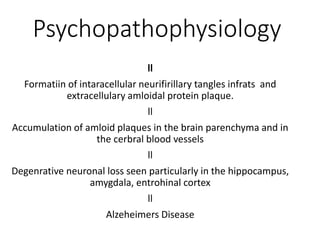
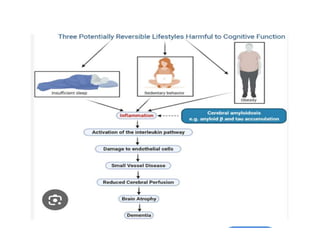
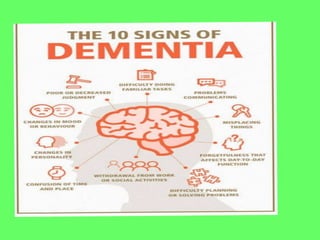

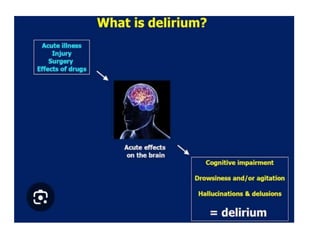
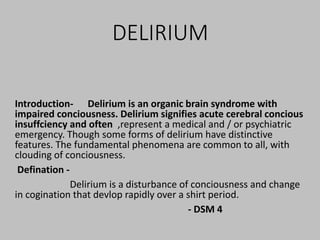
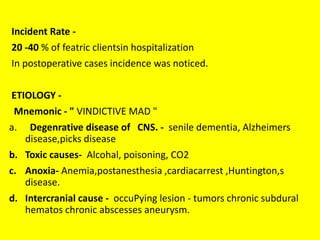
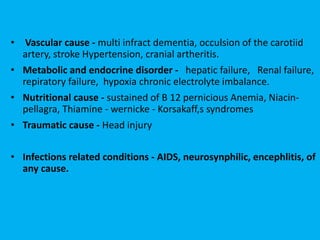
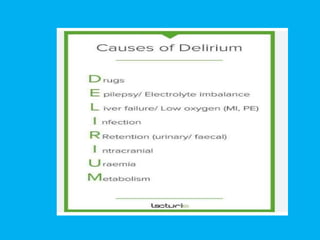

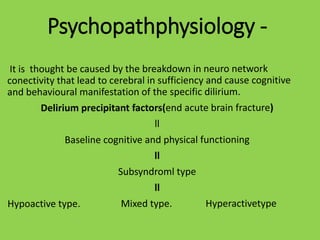
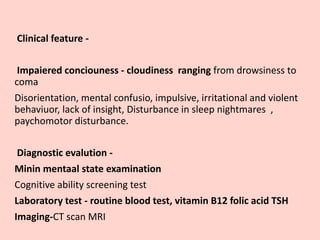




The document discusses organic mental disorders, including acute and chronic forms, as well as dementia, which is characterized by a decline in cognitive function due to various underlying diseases. It outlines classifications, incidence rates, common causes, and diagnostic evaluations for these disorders, emphasizing the need for appropriate medical management. The document also highlights specific types of dementia and delirium, presenting their distinct features and diagnostic criteria.















































![DELIRIUM_&_DEMENTIA[1]_Ngoma.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/deliriumdementia1ngoma-231022110253-0a2f4eb8-thumbnail.jpg?width=640&height=640&fit=bounds)
![NURSING CARE PLAN.doc [PSYCHATRIC PATIENT]](https://cdn.slidesharecdn.com/ss_thumbnails/nursingcareplan-250325094815-f3ace806-thumbnail.jpg?width=640&height=640&fit=bounds)
![nursing care plan.docx [MHN] PSYCHATRIC PATIENT](https://cdn.slidesharecdn.com/ss_thumbnails/nursingcareplan-250325094427-b1d61f11-thumbnail.jpg?width=640&height=640&fit=bounds)



![process 2.docx (FORMAT )[MENTAL HEALTH NURISNG ASSIGNMENT]](https://cdn.slidesharecdn.com/ss_thumbnails/process2-250325092750-d08f0852-thumbnail.jpg?width=640&height=640&fit=bounds)


![Genetic counselling.pptx [M.Sc Nursing I y]](https://cdn.slidesharecdn.com/ss_thumbnails/geneticcounselling-250311060616-f1112afb-thumbnail.jpg?width=640&height=640&fit=bounds)


![Chromosomes.pptx(Nursing) M.Sc [ Advance health Nurisng]](https://cdn.slidesharecdn.com/ss_thumbnails/chromosomes-250311055126-ad865c01-thumbnail.jpg?width=640&height=640&fit=bounds)



























