Download as DOC, PPTX
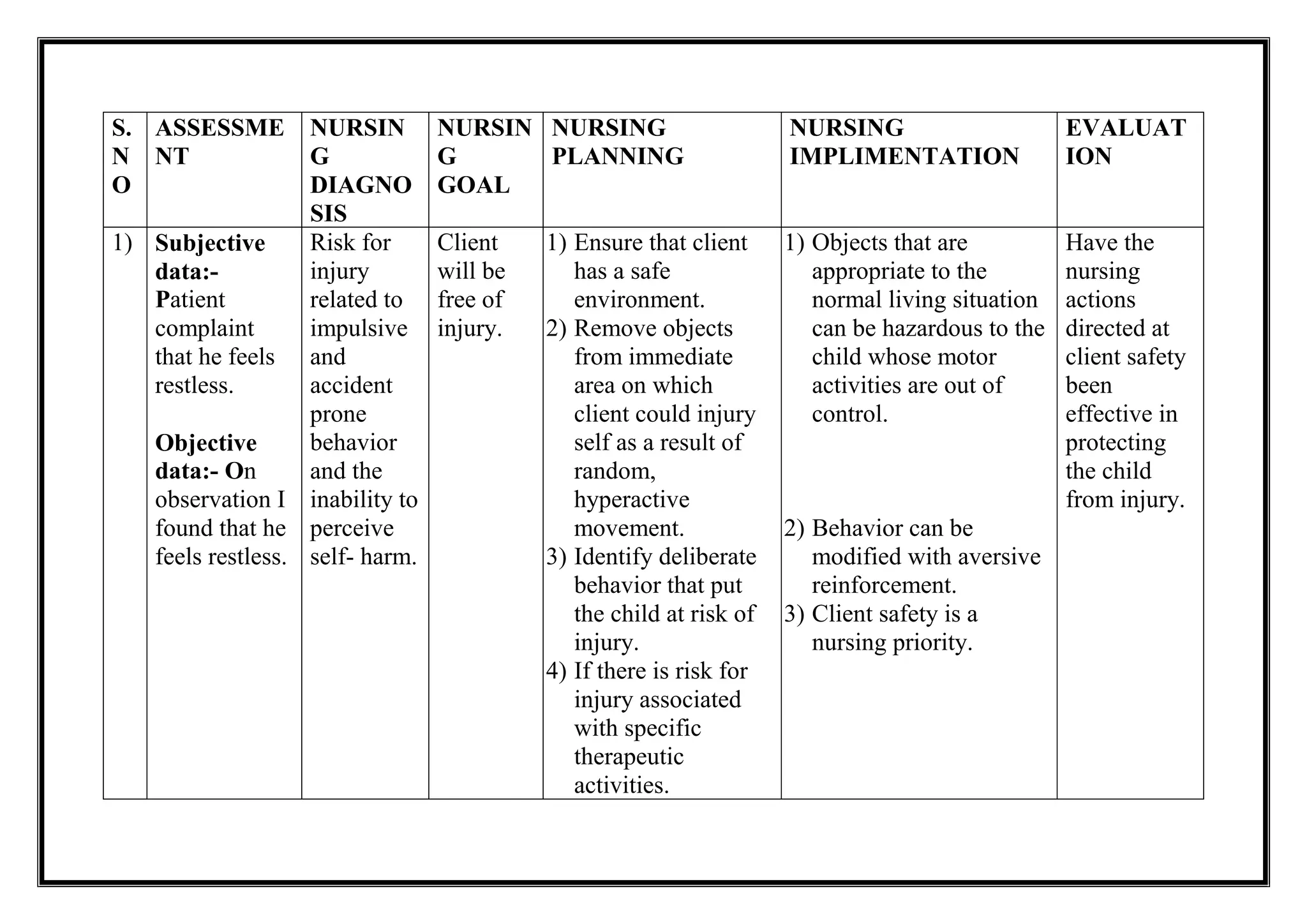
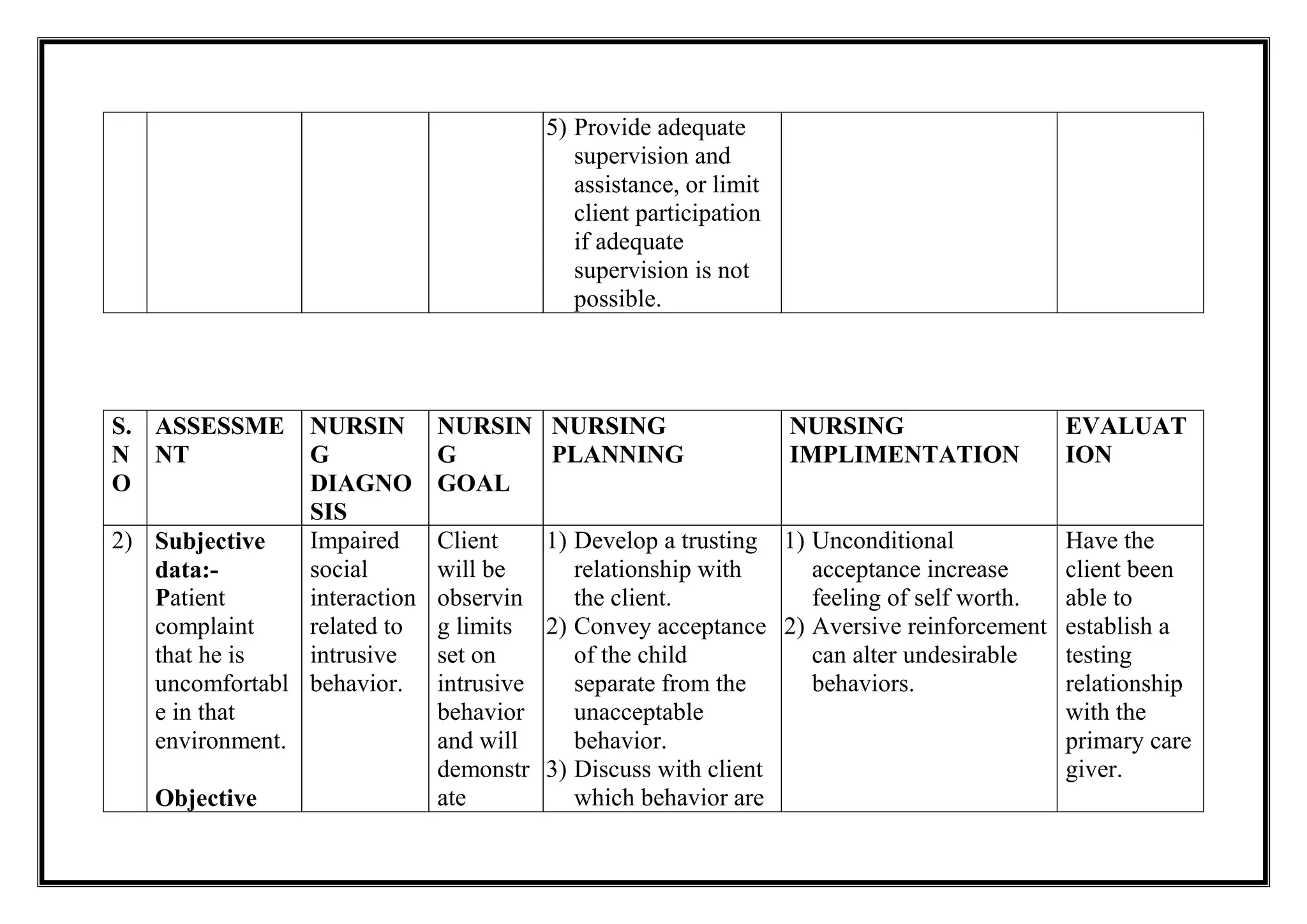



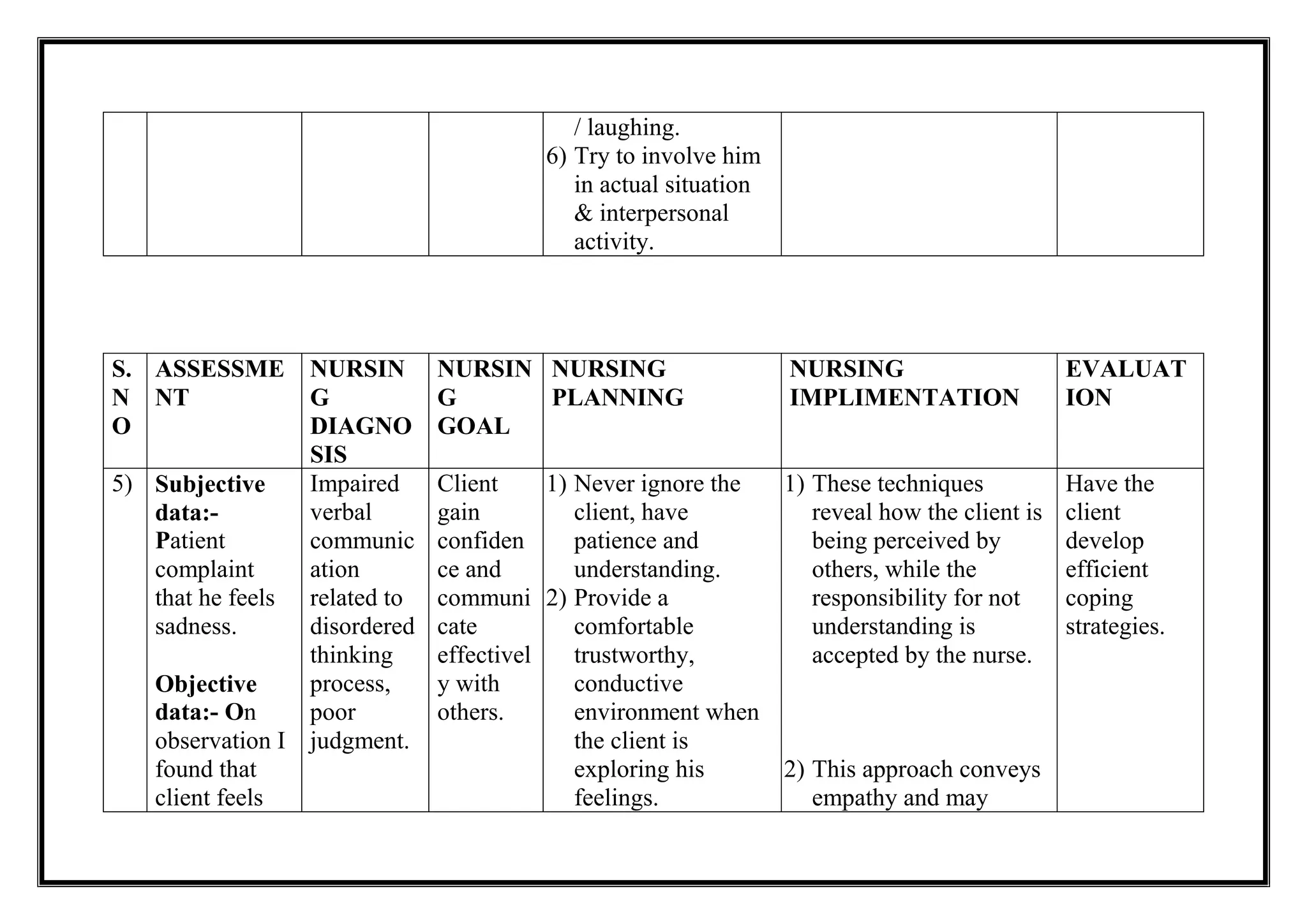


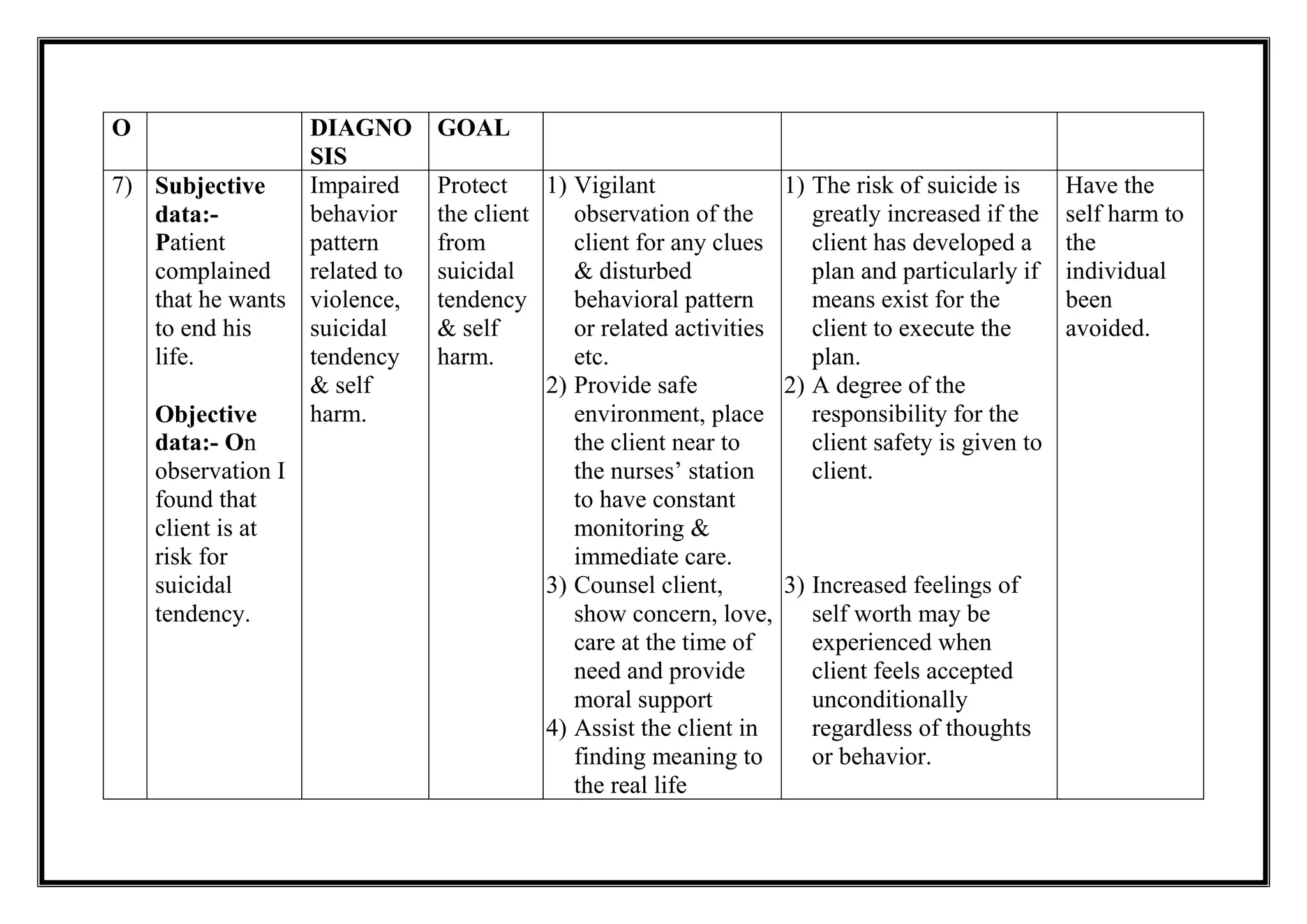




The document outlines a nursing assessment and care plan for patients exhibiting various psychological and behavioral issues, including restlessness, low self-esteem, impaired communication, and suicidal tendencies. It emphasizes the importance of creating a safe environment, building therapeutic relationships, and using positive reinforcement to promote desired behaviors. Additionally, strategies for improving social interactions, coping mechanisms, and self-care management are detailed to enhance patients' overall well-being.


































![NURSING CARE PLAN.doc [PSYCHATRIC PATIENT]](https://cdn.slidesharecdn.com/ss_thumbnails/nursingcareplan-250325094815-f3ace806-thumbnail.jpg?width=640&height=640&fit=bounds)









![nursing care plan.docx [MHN] PSYCHATRIC PATIENT](https://cdn.slidesharecdn.com/ss_thumbnails/nursingcareplan-250325094427-b1d61f11-thumbnail.jpg?width=640&height=640&fit=bounds)













![Genetic counselling.pptx [M.Sc Nursing I y]](https://cdn.slidesharecdn.com/ss_thumbnails/geneticcounselling-250311060616-f1112afb-thumbnail.jpg?width=640&height=640&fit=bounds)
![Chromosomes.pptx(Nursing) M.Sc [ Advance health Nurisng]](https://cdn.slidesharecdn.com/ss_thumbnails/chromosomes-250311055126-ad865c01-thumbnail.jpg?width=640&height=640&fit=bounds)





![process 2.docx (FORMAT )[MENTAL HEALTH NURISNG ASSIGNMENT]](https://cdn.slidesharecdn.com/ss_thumbnails/process2-250325092750-d08f0852-thumbnail.jpg?width=640&height=640&fit=bounds)





















