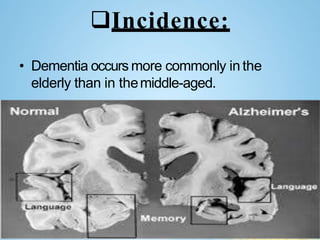
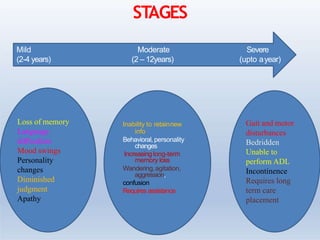
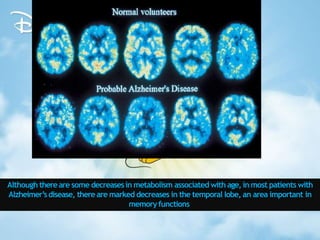
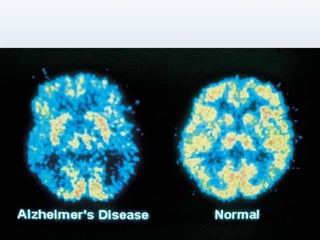
Dementia is a chronic organic brain syndrome characterized by global cognitive impairment. It is most commonly seen in the elderly and causes include Alzheimer's disease and vascular dementia. Dementia is classified and progresses through mild, moderate, and severe stages. Symptoms include memory loss, problems with language and tasks, and changes in mood and behavior. Diagnosis involves cognitive assessments and imaging tests. Treatment focuses on medications to improve symptoms and nursing management of daily care, safety, and emotional support for patients and their families.