This document provides an overview of optic neuritis, including its:
- Anatomy of the optic nerve and its coverings.
- Microscopy and physiology of the optic nerve.
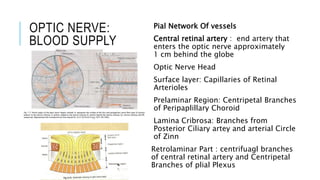
- Blood supply to the optic nerve.
- Parts of the optic nerve from intracanalicular to intracranial segments.
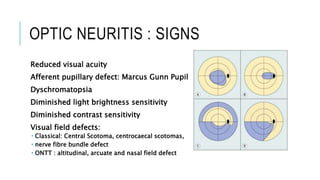
- Clinical features, signs, investigations, and treatment of optic neuritis, including results from the Optic Neuritis Treatment Trial.