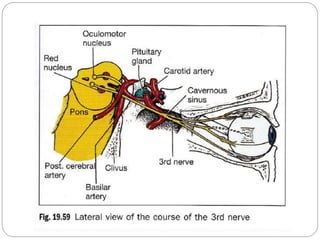
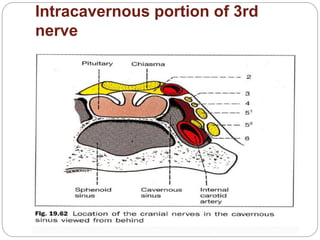
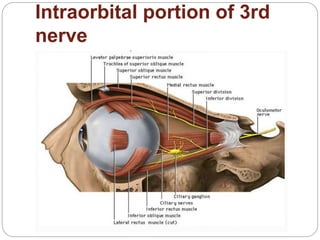
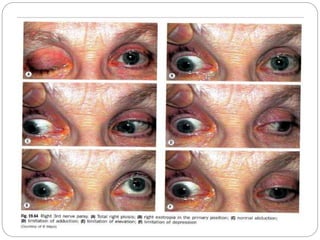
The document discusses the oculomotor nerve (cranial nerve 3), which is entirely motor and supplies several extraocular muscles and the levator palpebrae superioris muscle. It has nuclei located in the midbrain and courses from the midbrain to the orbit. Common causes of cranial nerve 3 palsy include vascular issues like diabetes and hypertension, neoplastic lesions, and trauma. Signs of a total cranial nerve 3 palsy include ptosis, limitation of eye movements, and a dilated pupil. Treatment depends on the underlying cause but may involve surgery, patching, or prism correction of double vision.