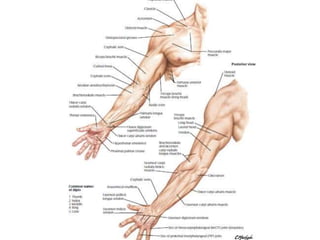
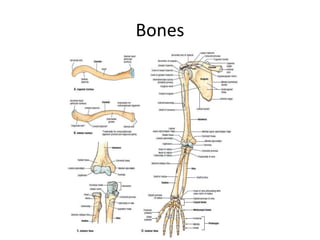
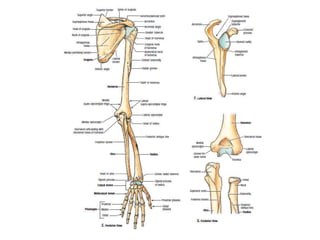
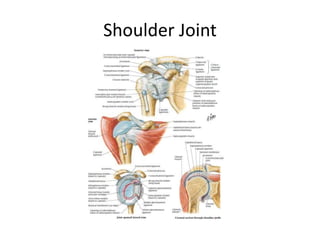
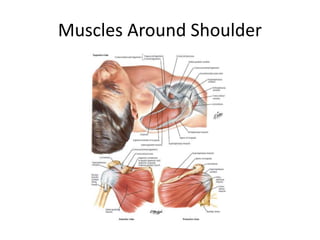
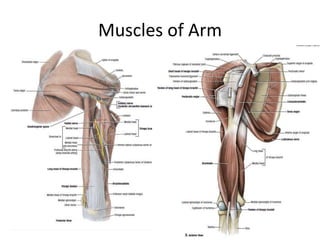
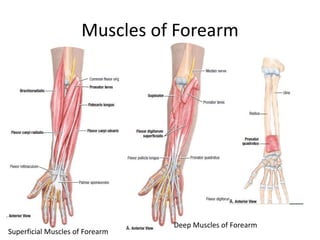
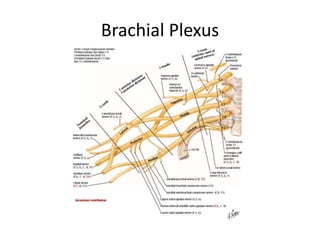
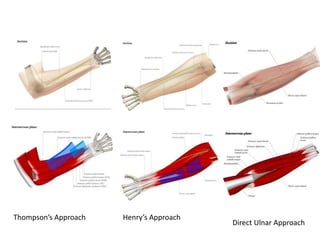
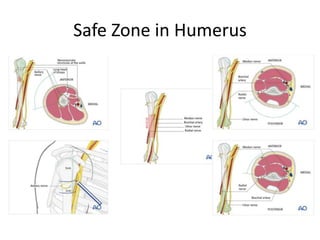
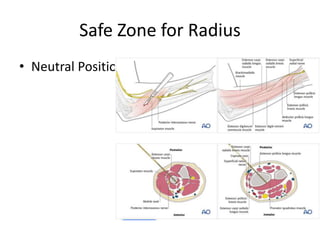
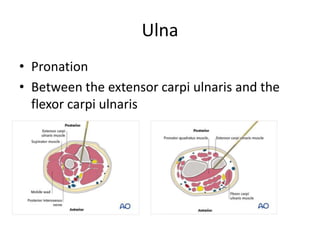
The document discusses the applied anatomy of the upper limb, covering topics such as its development, surface anatomy, bones, joints, muscles, and neurovascular structures. It also highlights common pathologies, surgical approaches, and injuries related to the upper limb, emphasizing the importance of understanding function alongside structure for effective clinical treatment. Key anatomical details, including the brachial plexus injuries and specific surgical techniques, are presented by Dr. Kaushal Raj Kafle under the moderation of Dr. Nischal Ghimire.








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











