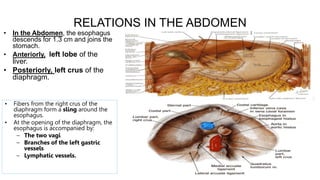
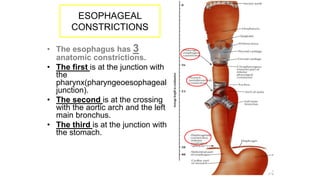
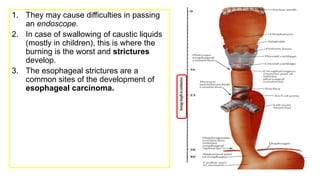
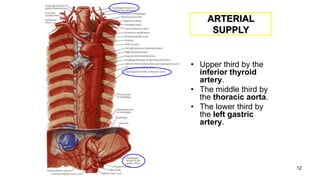
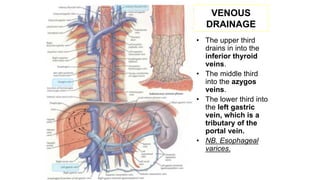
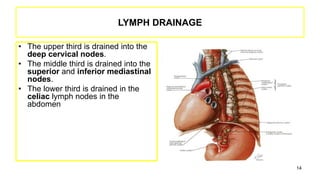
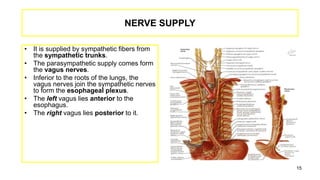
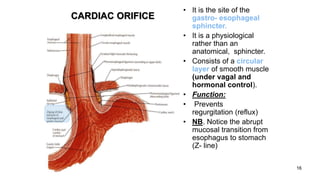
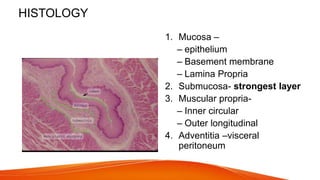
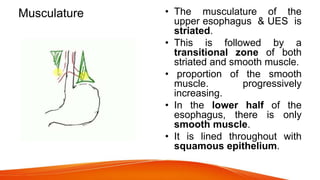
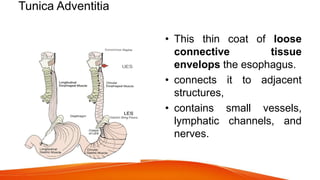
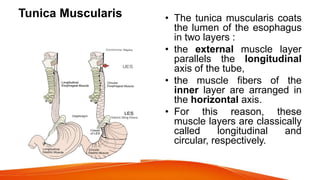
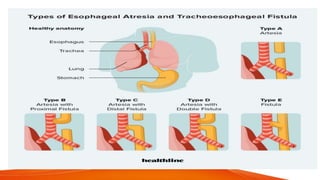
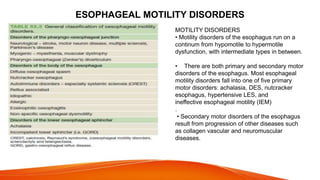
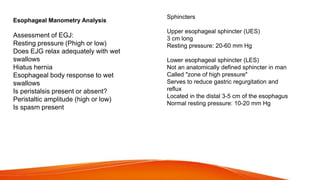
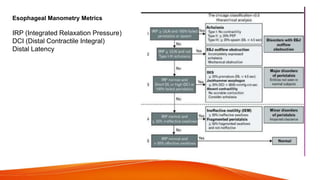
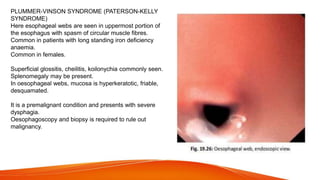
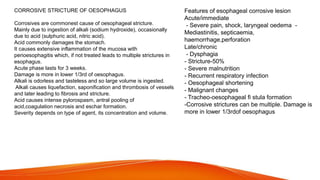
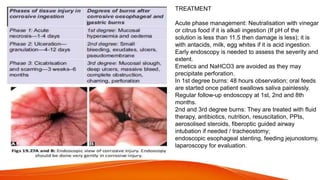
The document outlines the surgical anatomy of the esophagus and its associated benign disorders, detailing its embryonic development, structure, and relations in the body. It discusses key aspects such as arterial supply, venous drainage, nerve supply, and common disorders like atresia, stenosis, hiatus hernia, and achalasia, including their symptoms and treatment options. The text emphasizes the importance of esophageal manometry in diagnosing motility disorders and the surgical interventions available for conditions like achalasia.