Download as PDF, PPTX



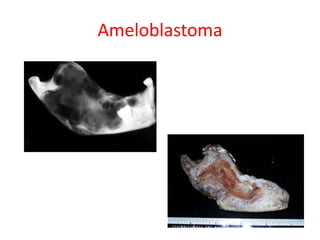
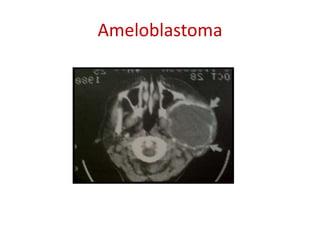
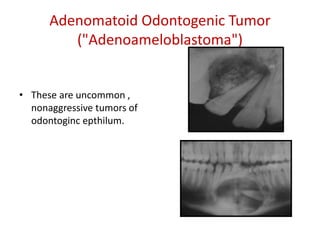
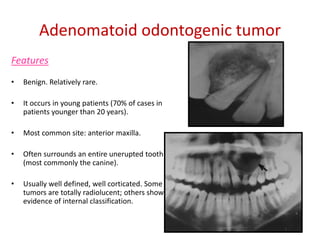
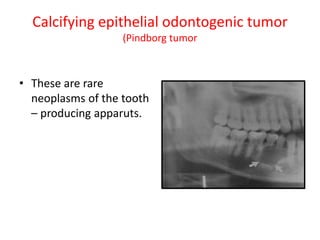
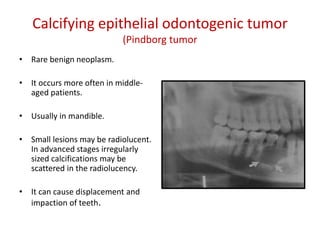
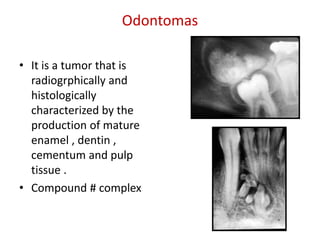
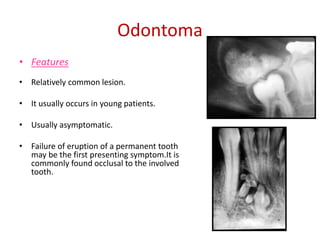
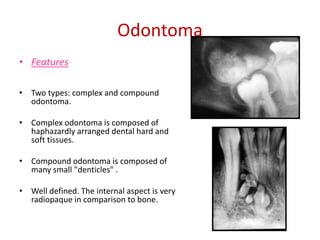
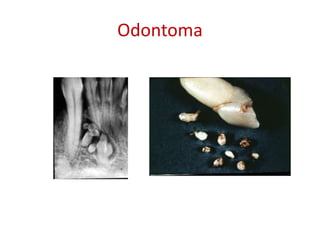
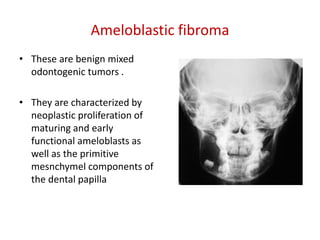
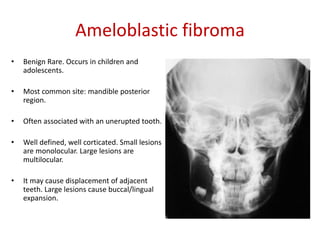
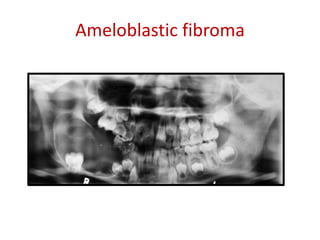









This document summarizes several odontogenic tumors including: ameloblastoma (benign, locally aggressive tumor of odontogenic epithelium that commonly occurs in the mandible), adenomatoid odontogenic tumor (uncommon, nonaggressive tumor that often surrounds an unerupted tooth), calcifying epithelial odontogenic tumor (rare benign neoplasm that usually occurs in the mandible), odontoma (tumor characterized by production of dental tissues that commonly occurs in young patients), ameloblastic fibroma (benign mixed odontogenic tumor that occurs in children/adolescents), odontogenic myxoma (benign tumor arising from dental papilla mesenchyme), cementoblast











































































