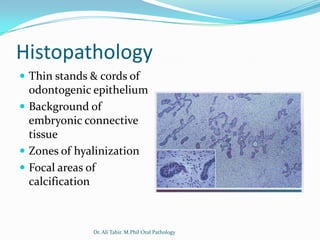
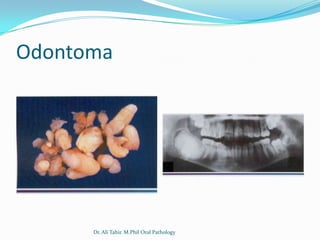
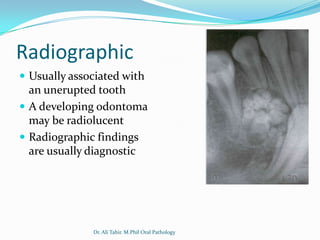
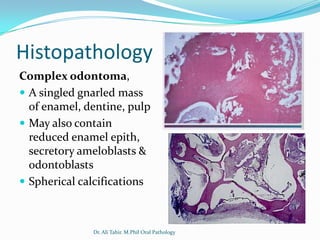
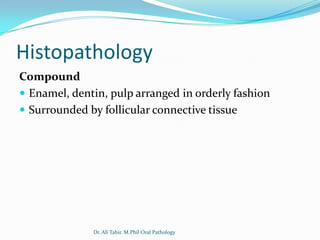

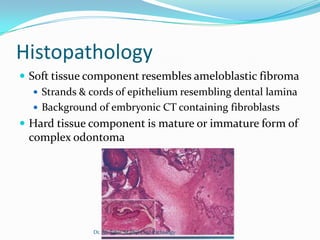
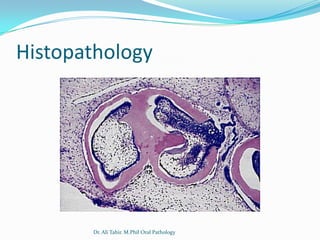


Ameloblastic fibroma is a benign odontogenic tumor that occurs in young patients. It consists of odontogenic epithelium and connective tissue, and is usually located in the mandibular molar region associated with unerupted teeth. Radiographically, it appears as a well-defined unilocular or multilocular radiolucency. Histologically, it contains thin strands and cords of odontogenic epithelium in an embryonic connective tissue background. Odontoma is the most common odontogenic tumor. It is a hamartoma composed of enamel, dentin, pulp and cementum in the form of tooth-like structures (compound) or a solid mass (















































































