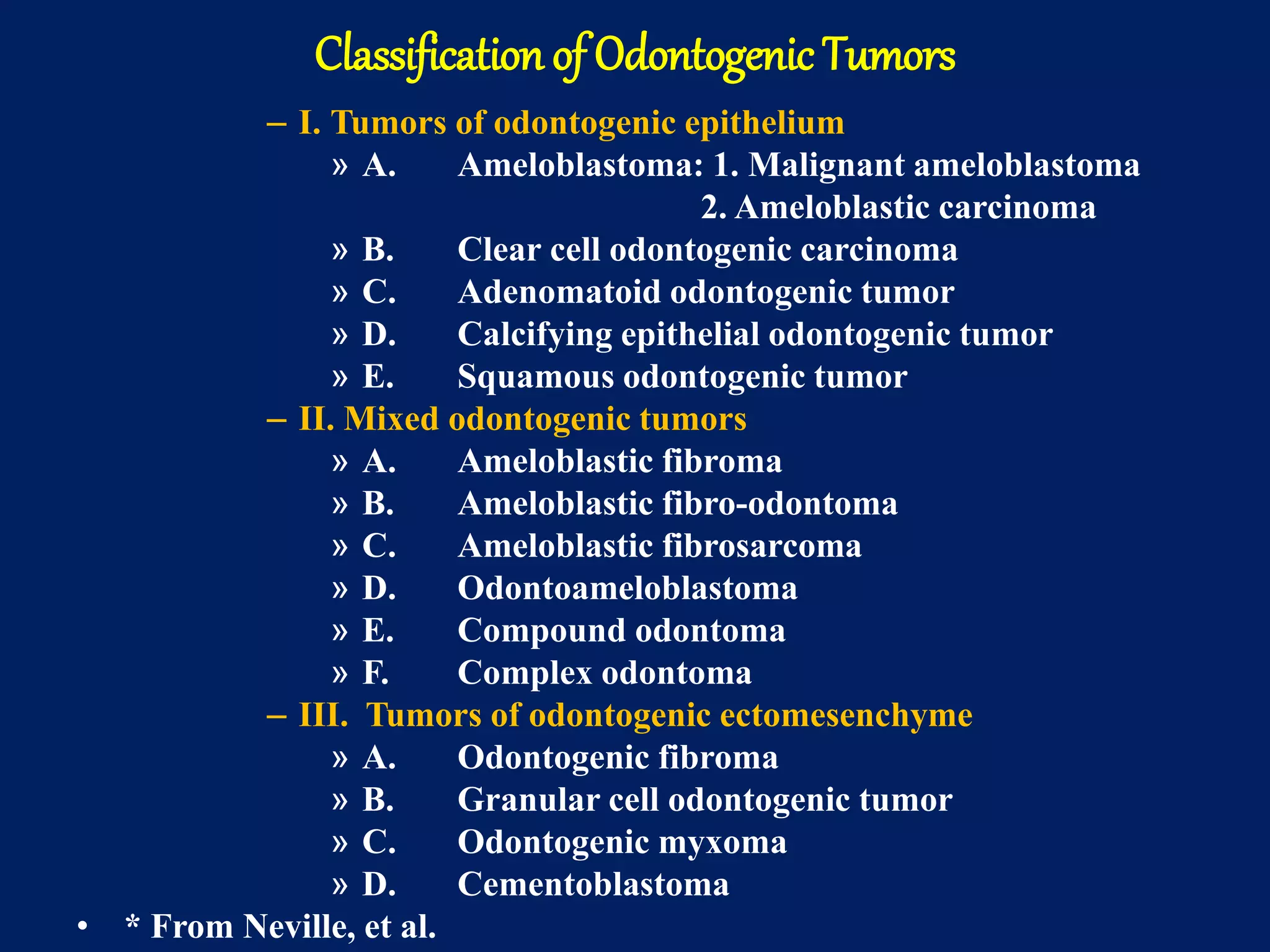
This document discusses different types of odontogenic tumors. It classifies them into three categories: tumors of odontogenic epithelium, mixed odontogenic tumors, and tumors of odontogenic ectomesenchyme. Key tumors discussed include ameloblastoma, adenomatoid odontogenic tumor (AOT), and calcifying epithelial odontogenic tumor (CEOT). Ameloblastoma is the most common odontogenic tumor and can be solid/multicystic, unicystic, or peripheral. AOT typically occurs in younger females in the anterior maxilla. CEOT accounts for less than 1% of odontogenic tumors and resembles cells of the enamel organ or dental lamina.