Downloaded 4,328 times






























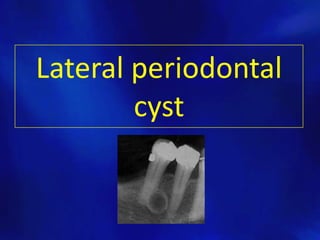









































The document outlines various types of odontogenic cysts, their classifications, causes, histopathology, clinical features, and treatment options. It discusses specific types of cysts such as radicular, residual, dentigerous, lateral periodontal, and odontogenic keratocysts, providing insights into their origins and radiographic characteristics. Treatment approaches include enucleation and marsupialization, tailored based on the cyst's characteristics and impact on surrounding structures.
























































![CystS in oral pathology dental edu[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cysts1-250430234019-1ab3f067-thumbnail.jpg?width=640&height=640&fit=bounds)

















































