Downloaded 571 times
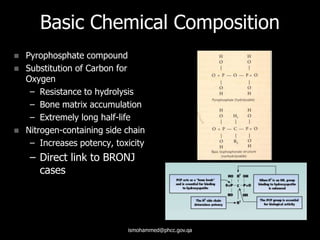








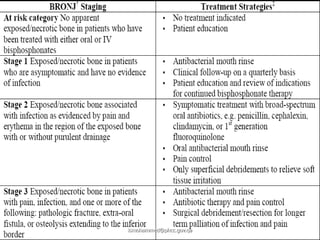

This document provides information on bisphosphonate-related osteonecrosis of the jaws (BRONJ). It begins with background on bisphosphonates, including their uses, mechanisms of action, and side effects. It then discusses the history, estimated incidence, risk factors, clinical presentation, staging, and treatment of BRONJ. The document aims to educate on this condition caused by prolonged bisphosphonate use that results in exposed bone in the jaw.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













