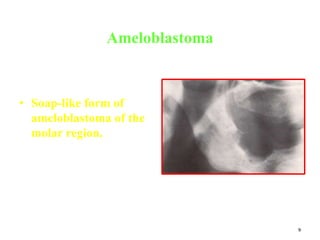
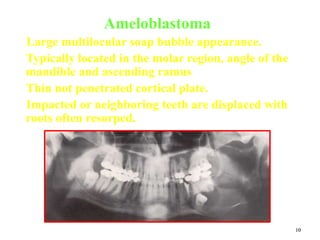
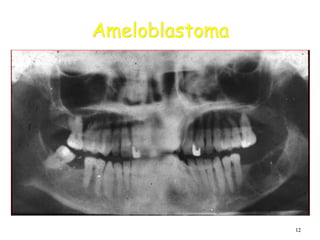
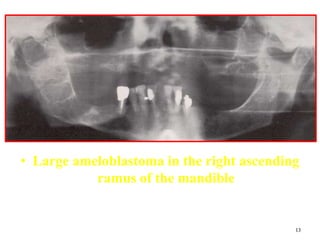
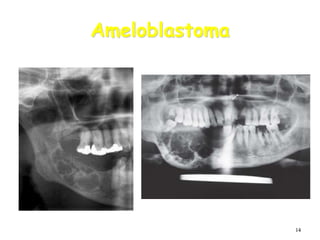
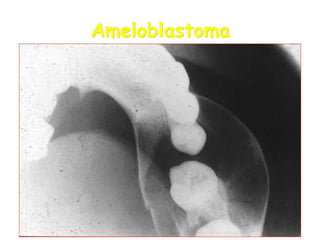
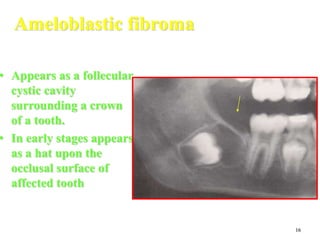
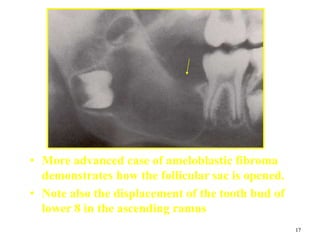
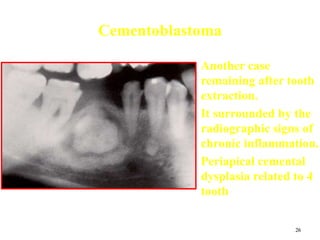
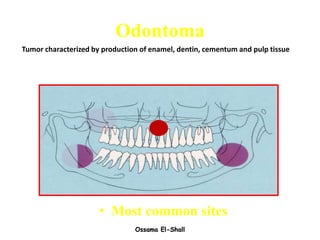
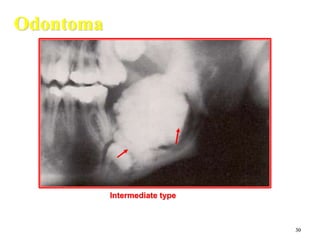
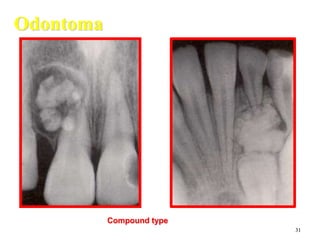
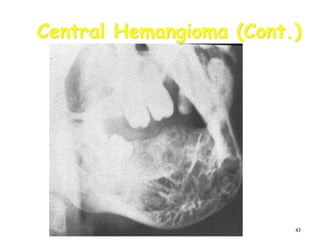
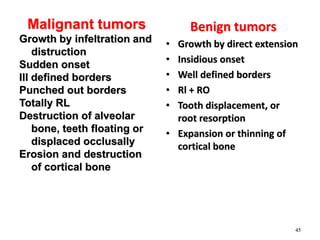
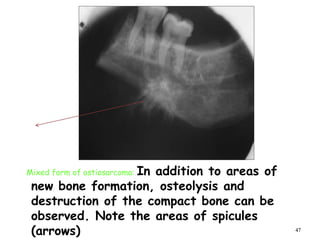
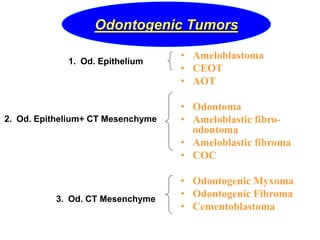
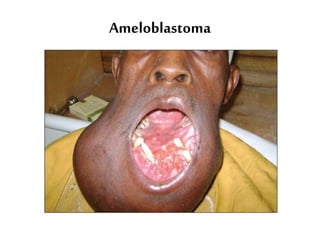
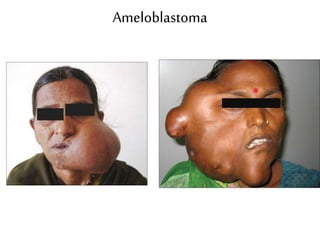
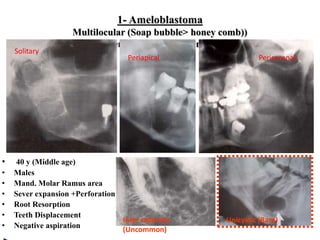
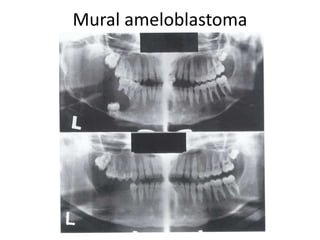
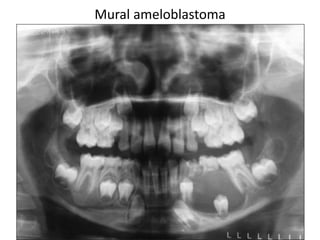
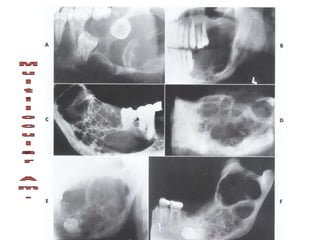
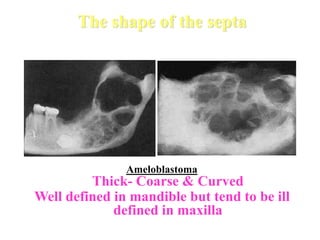
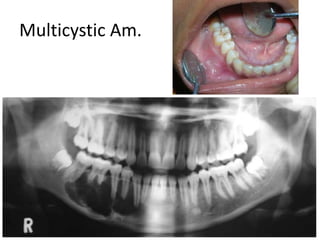
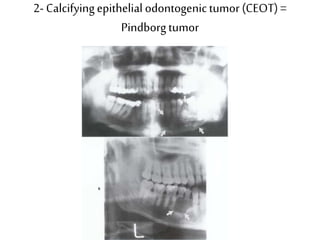
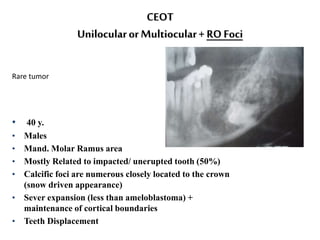
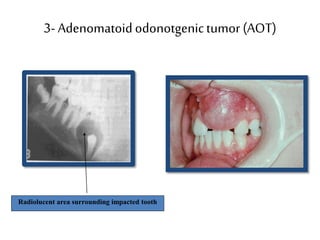
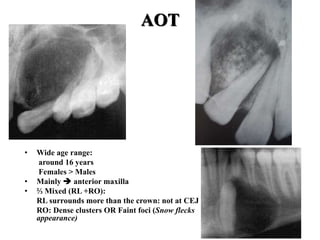
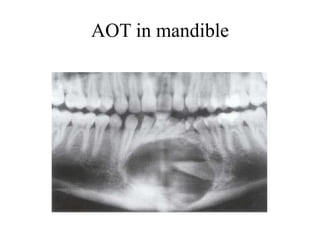
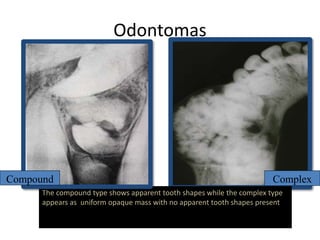
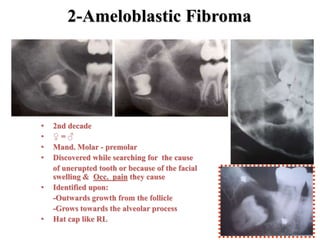
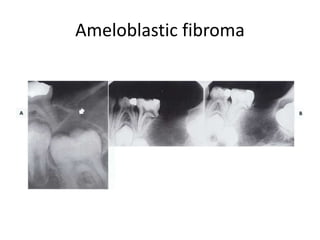
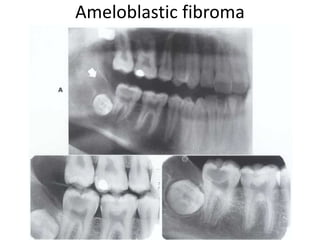
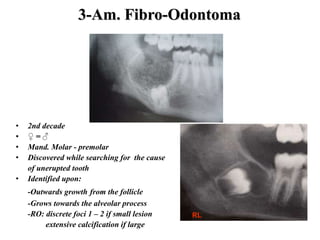
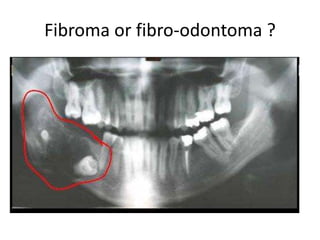
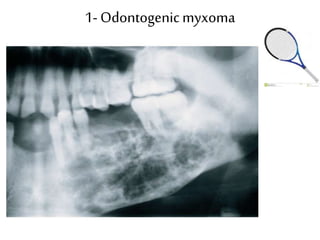
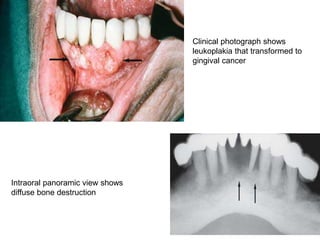
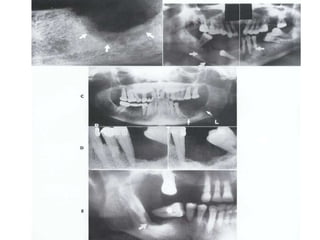
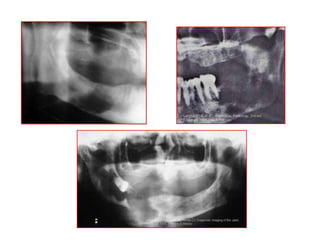
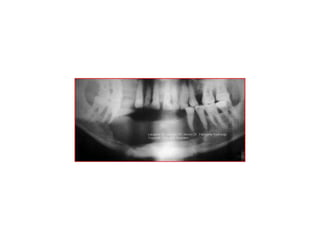
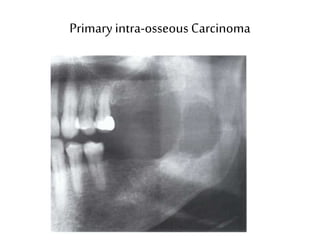
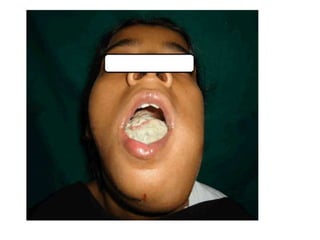
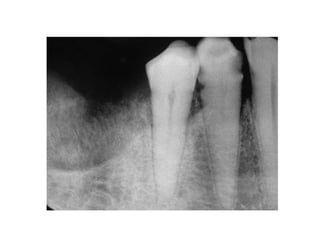
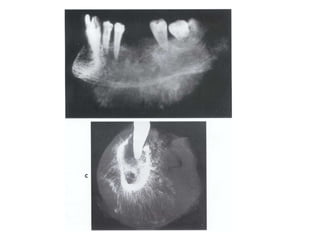
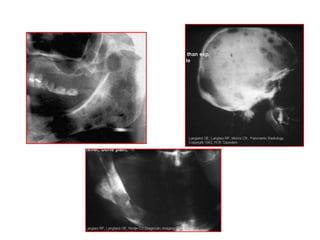
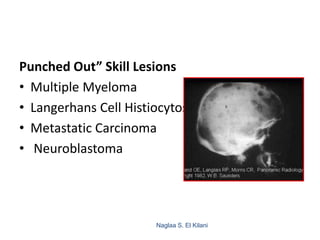
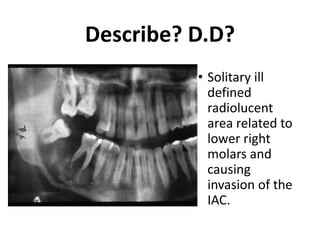
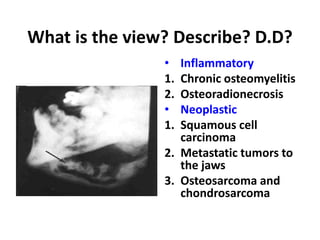
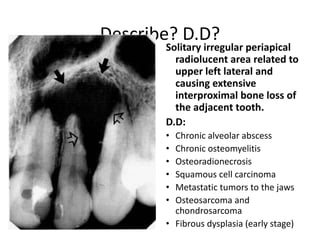
The document discusses various odontogenic and non-odontogenic tumors seen radiographically, including details on ameloblastoma, CEOT, AOT, odontoma, and central hemangioma among others. Malignant tumors such as osteosarcoma are also covered, describing features such as bone destruction, osteolysis, and the sunray periosteal reaction. Differential diagnoses are provided for many of the lesions based on characteristics such as location, borders, tooth involvement, and expansion or destruction of bone.