
































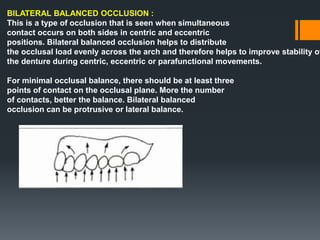

















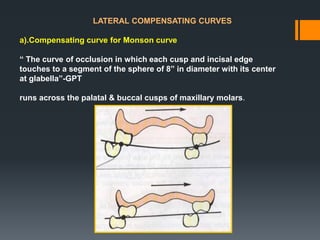

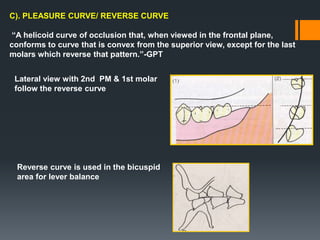





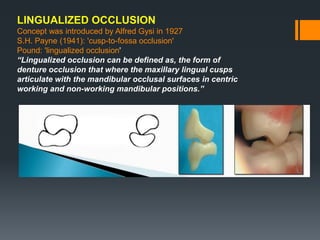













The document discusses various concepts related to complete denture occlusion including: - The history of dental occlusion in mammals and its development. - Andrews' six keys to normal occlusion which are seen in natural dentition. - Differences between natural tooth occlusion and artificial denture occlusion. - Various occlusal schemes for complete dentures including balanced, lingualized, and monoplane occlusion. - Requirements for incisive, working, and balancing units in occlusal schemes.

























































![]Dental Occlusion part 1](https://cdn.slidesharecdn.com/ss_thumbnails/occlusionpart1-160420073612-thumbnail.jpg?width=640&height=640&fit=bounds)






















