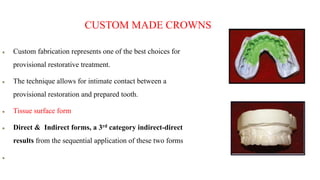
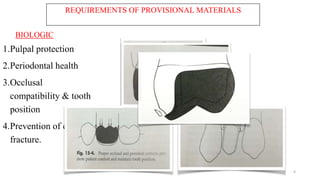
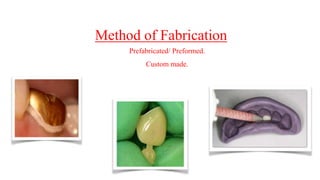
This document discusses provisional restorations in fixed partial dentures. It defines provisional restorations and outlines their requirements including biologic, mechanical, and esthetic considerations. It classifies provisional restorations by fabrication method, technique, location, and duration of use. Common materials used include resin-based and metal provisionals. Fabrication techniques include direct, indirect, and indirect-direct. Provisional cements and their uses are also covered. The document discusses applications of provisional restorations in laminates and implant dentistry and concludes with limitations and recent advances.

![CELLULOSE ACETATE:
Thin [0.2 – 0.3 mm] transparent material.
Available in all tooth types and range of sizes.
Do not chemically or mechanically bond to the inside surface so after polymerisation the
shell is peeled off.
The disadvantages are :
• They merely act as a matrix and so must be removed after their relining material has set.
• When the cellulose crown form is removed, the thickness of the crown get reduced (by
about 0.2 mm). This may lead to instability in the occlusion and movement of adjacent teeth.](https://image.slidesharecdn.com/provisionalrestoration-1-240304163734-2c4023f6/85/provisional-restoration-fixed-partial-denture-12-320.jpg)