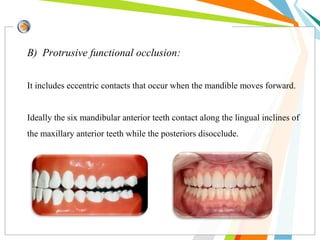
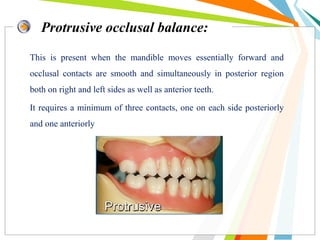
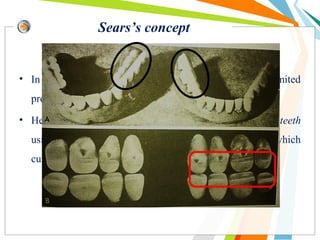
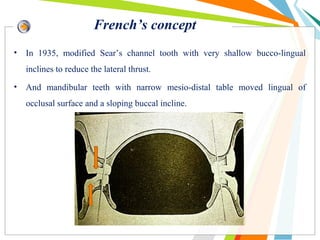
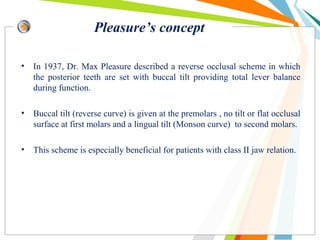
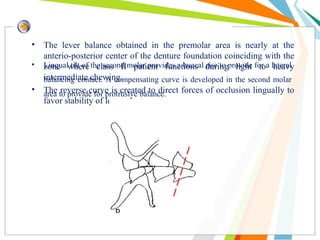
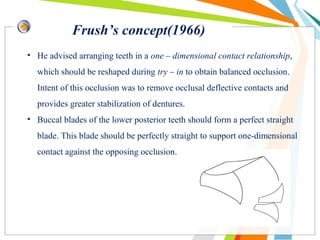
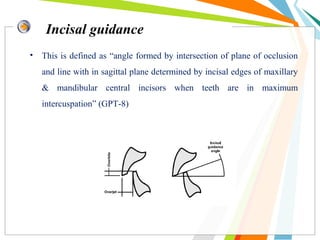
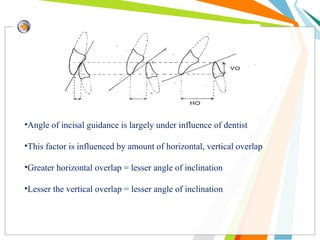
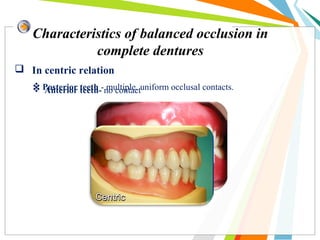
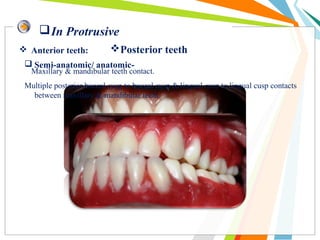
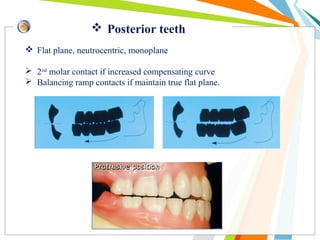
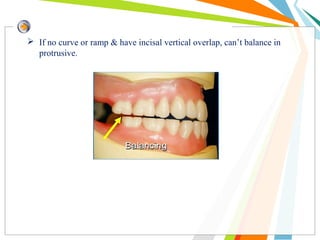
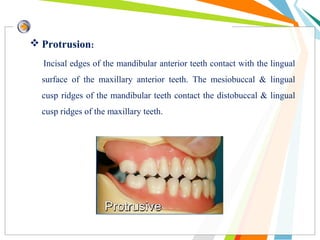
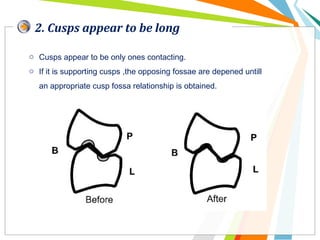
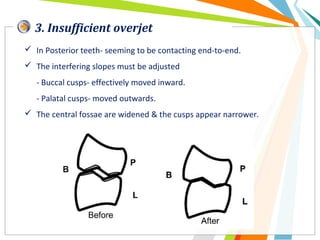
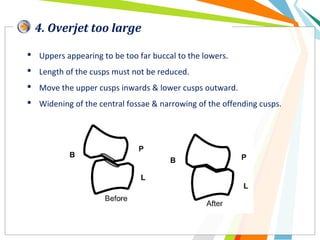
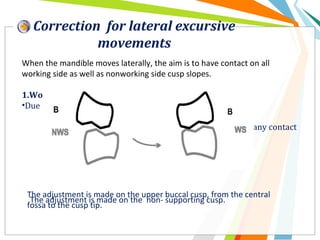
This document provides an overview of balanced occlusion and its importance in complete denture fabrication. It defines key terms like balanced occlusion, centric occlusion, eccentric occlusion, and discusses various theories of occlusion. It describes the requirements and goals of balanced occlusion in complete dentures. Various concepts of balanced occlusion are outlined, including those proposed by Gysi, Sears, French, Pleasure, Frush, Hanau and others. The document discusses the advantages of bilateral balanced occlusion and factors that affect achieving balanced occlusion in complete dentures.