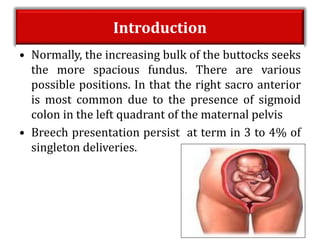
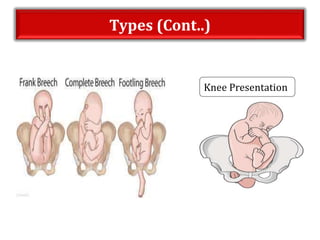
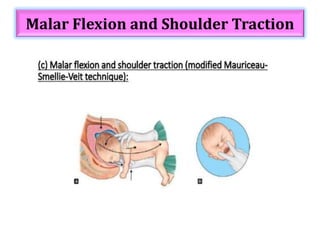
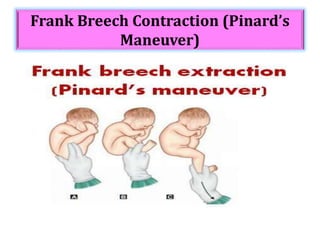
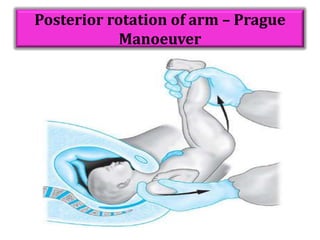
Breech presentation occurs when the fetus lies longitudinally with the pelvic or podalic pole presenting at the birth canal instead of the head. It has an incidence of 3-15% depending on gestational age. There are various types of breech including complete, frank, and footling. Breech delivery can be managed through external cephalic version, vaginal delivery, or cesarean section depending on the fetal position and other risk factors. Vaginal breech delivery requires skilled assistance and maneuvers to safely deliver the fetus in stages starting with the buttocks and hips, shoulders, and finally the head. Complications for mother and baby can include injuries if not properly managed.