Downloaded 43 times


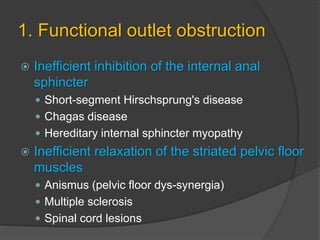
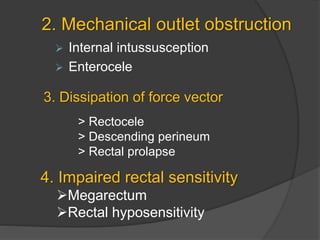
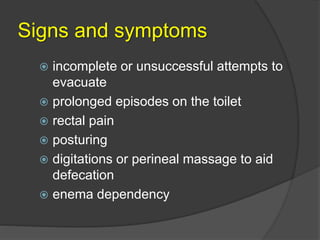


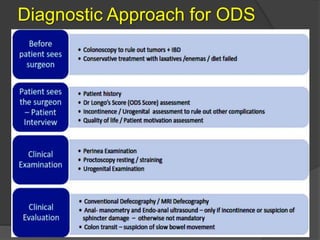
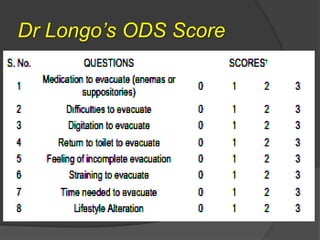
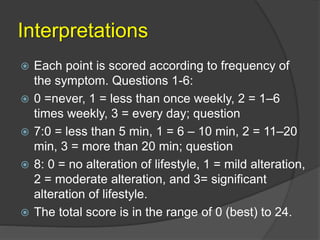
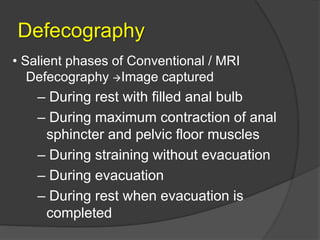
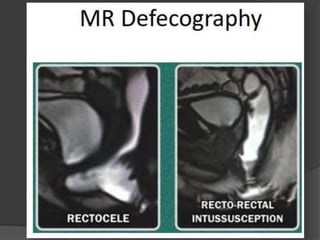





This document discusses obstructed defecation syndrome (ODS). It defines ODS as difficulty evacuating the rectum that may be associated with constipation. Common causes include diet, medications, and pelvic floor disorders. ODS is caused by abnormal function of muscles involved in defecation or anatomical abnormalities of pelvic organs. Diagnosis involves questionnaires, tests like defecography, and the ODS score. Treatment depends on the underlying cause and may include conservative options, biofeedback, or surgical procedures like STARR to repair defects.























































































