This document discusses several nutritional problems in public health, including:
- Low birth weight, protein energy malnutrition, xerophthalmia, nutritional anemia, iodine disorders, endemic fluorosis, and lathyrism.
- Low birth weight is an important public health issue as it is associated with higher risks of mortality, developmental issues, and other health problems. Prevention focuses on improving nutrition and health of women during pregnancy.
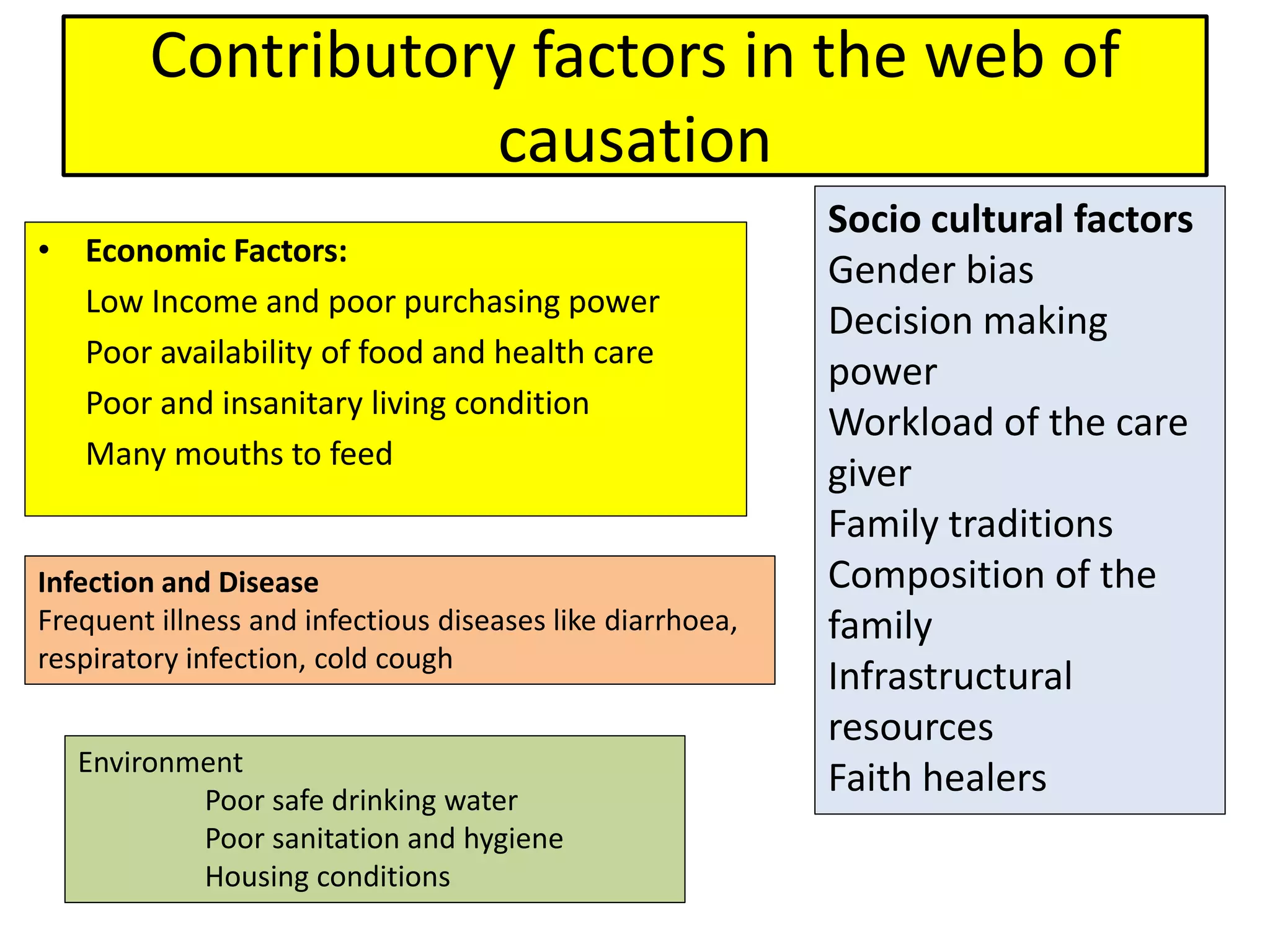
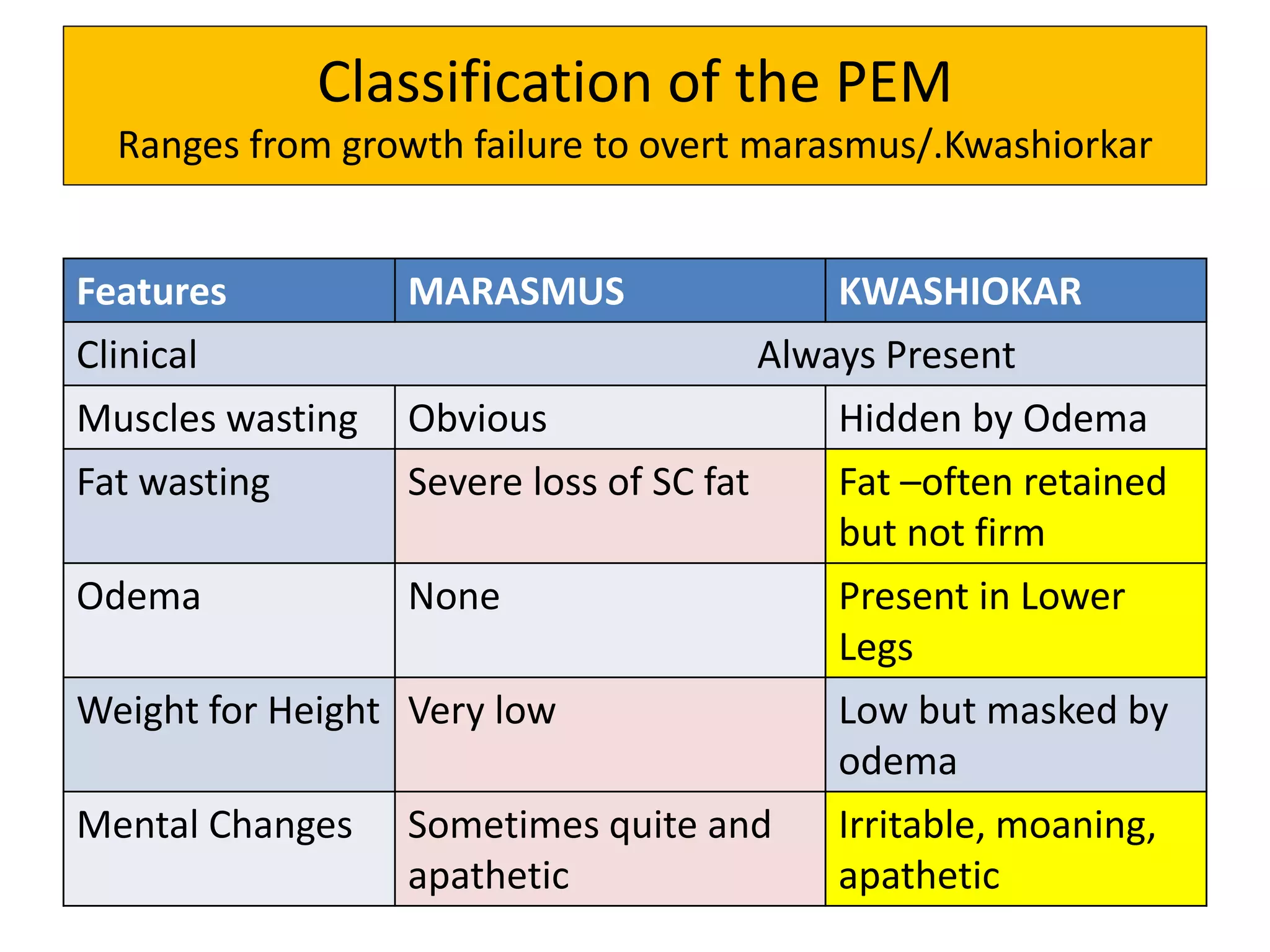
- Protein energy malnutrition includes conditions like marasmus and kwashiorkor and is caused by inadequate dietary intake of protein and energy. Prevention involves improving access to nutritious foods, treating infections, and nutritional rehabilitation programs.
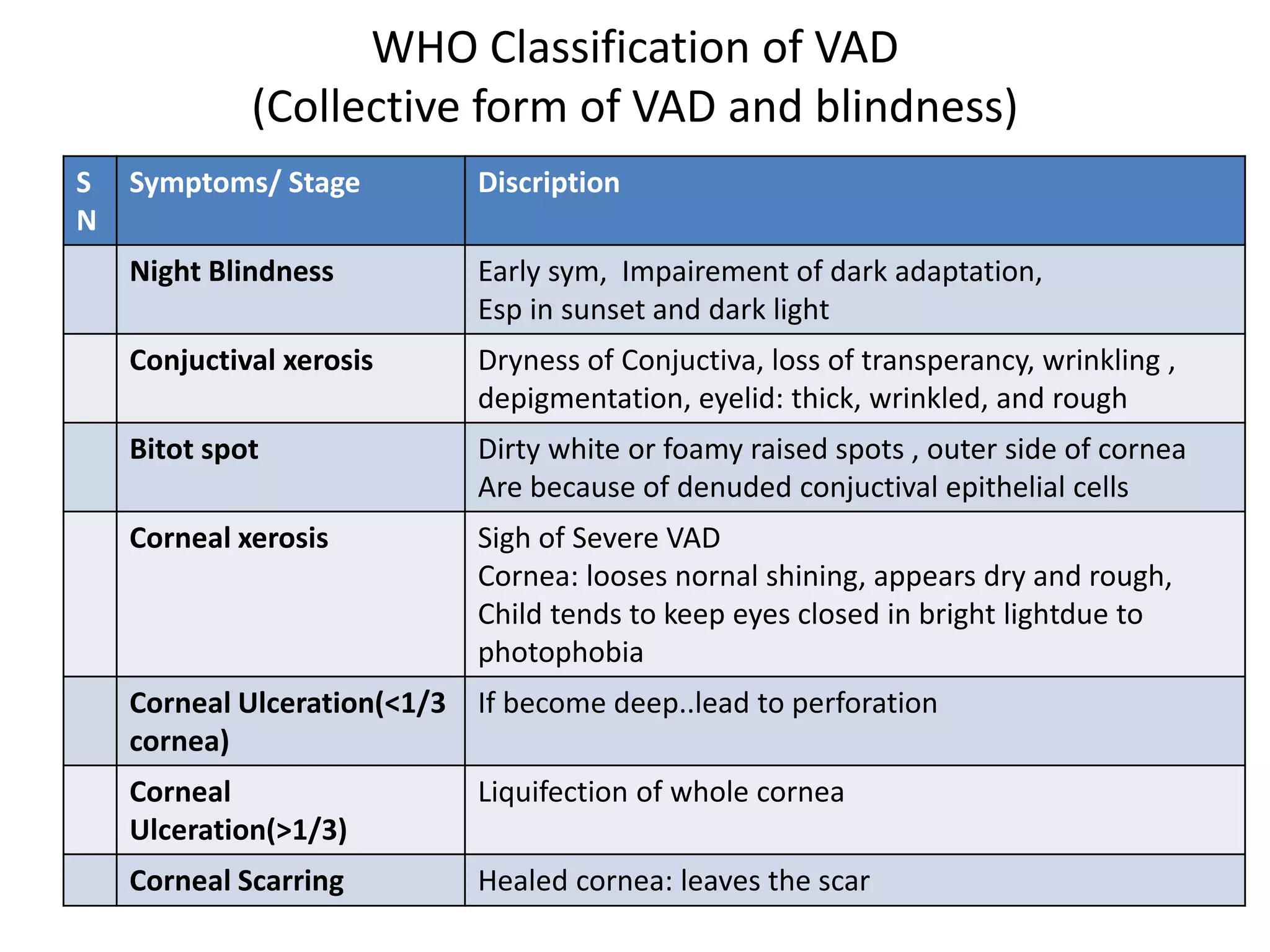
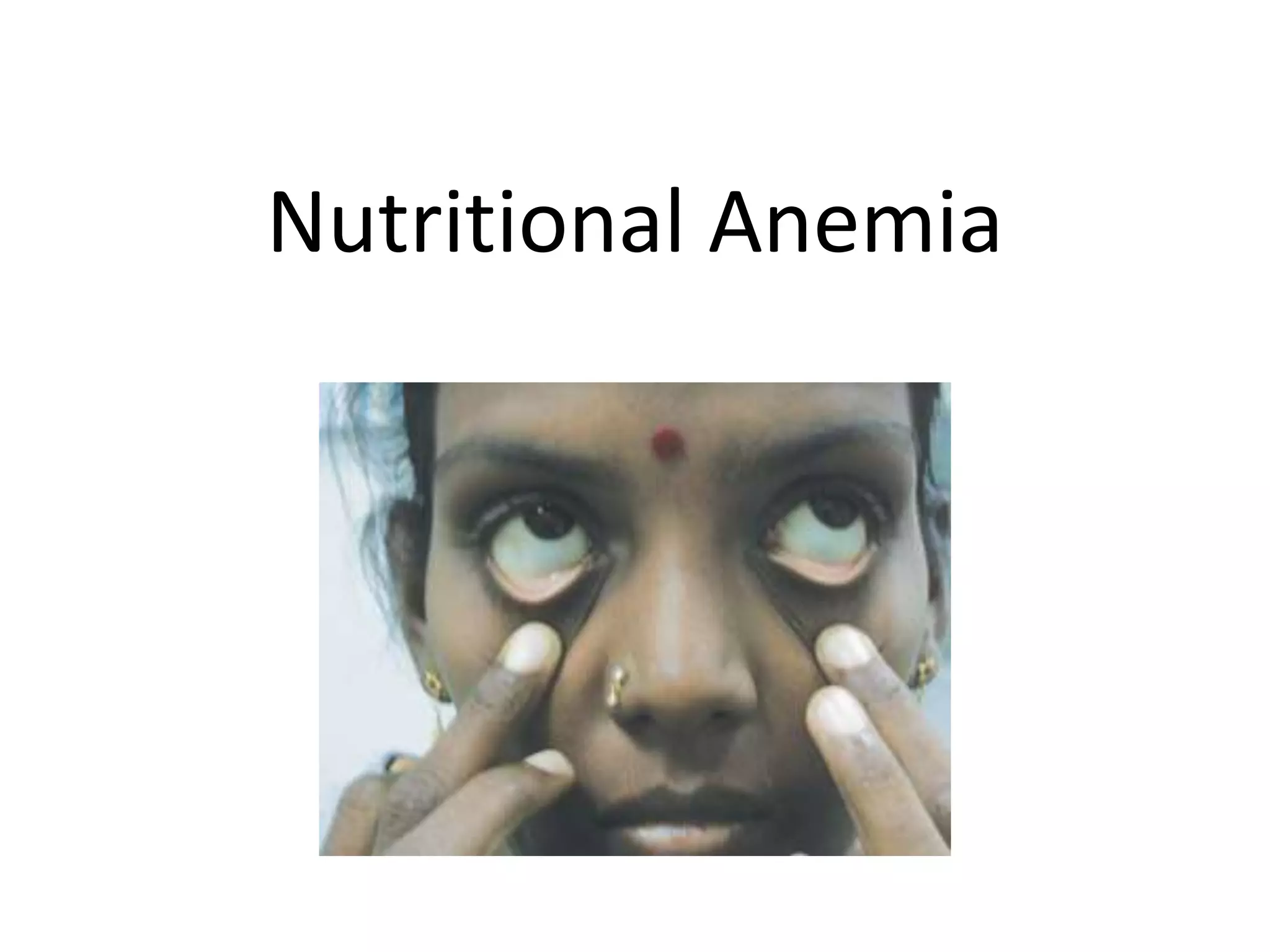
- Several micronutrient deficiencies