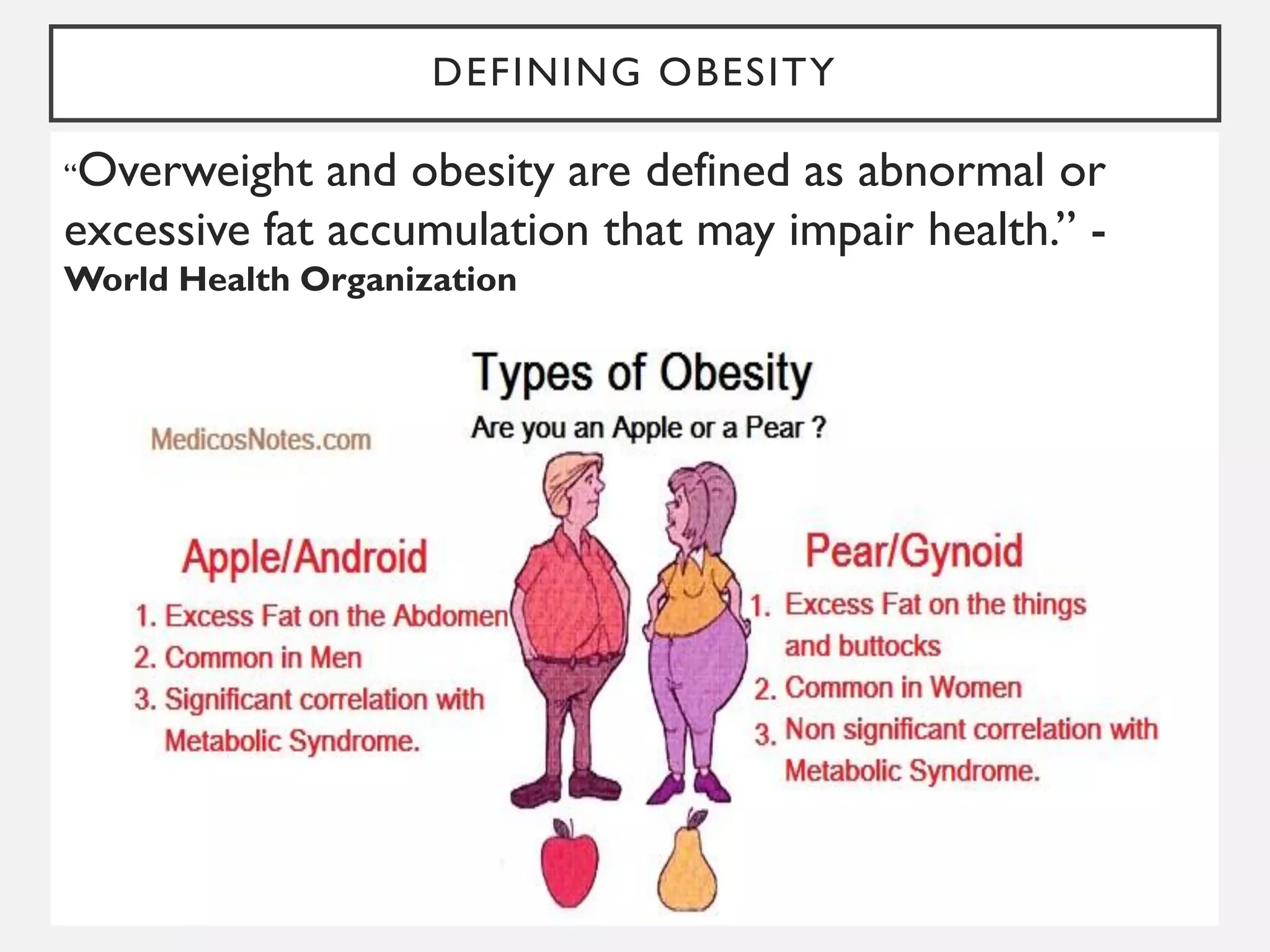
This document discusses obesity, including its definition, classification, epidemiology, morbidity and mortality, assessment and measurements, prevention and management, and addressing barriers. Obesity is defined as abnormal or excessive fat accumulation that may impair health. It is classified based on body mass index (BMI) and other criteria. Globally, obesity rates have significantly increased over recent decades and are associated with increased risk of diseases such as heart disease, diabetes and some cancers. Assessment methods include BMI, waist circumference, skin fold thickness and other measurements. Prevention and management involves diet, exercise, weight loss medications and sometimes surgery. Addressing obesity requires efforts across multiple levels including individual lifestyle changes, community programs, and national policies.






















![ASSESSMENT & MEASUREMENTS OF OBESITY
WEIGHT: HEIGHT RATIO (WHTR) :
• WHO has declared WHt Ratio as ‘best indicator of cardiovascular risk’
• WHtR is ‘age and sex independent’
• Cut-off for WHtR: 0.5
• CVD risk increase if WHtR >0.5
[NEW INDICATOR OF CV RISK by WHO]
OTHER INDICATORS:
• Total body water
• Total body potassium
• Body density
• Measurement of fat cells in the
body.](https://image.slidesharecdn.com/obesity-230710145705-e58fe7a8/75/Obesity-pdf-25-2048.jpg)























































![Obesity by bijay [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesitybybijayautosaved-200407031519-thumbnail.jpg?width=640&height=640&fit=bounds)

![Epidemiology of Obesity [Global and Indian Scenario]]](https://cdn.slidesharecdn.com/ss_thumbnails/epidemiologyofobesity-241217054751-c5a2ec52-thumbnail.jpg?width=640&height=640&fit=bounds)






















