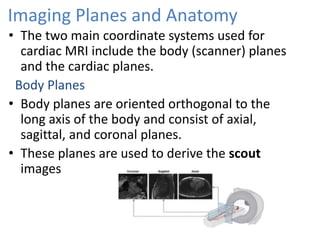
This document summarizes heart embryology and radiological anatomy. It describes how the heart develops from mesenchymal cell clusters that form the primitive heart tube. This tube undergoes looping and partitioning to form the four chambers. Endocardial cushions develop and divide the atrioventricular canal and outflow tract. The document then describes heart anatomy and landmarks seen on imaging modalities like ultrasound, CT and MRI. It details the structures of the atria, ventricles, valves and coronary arteries. Standard views used in echocardiography are also mentioned.