Downloaded 809 times

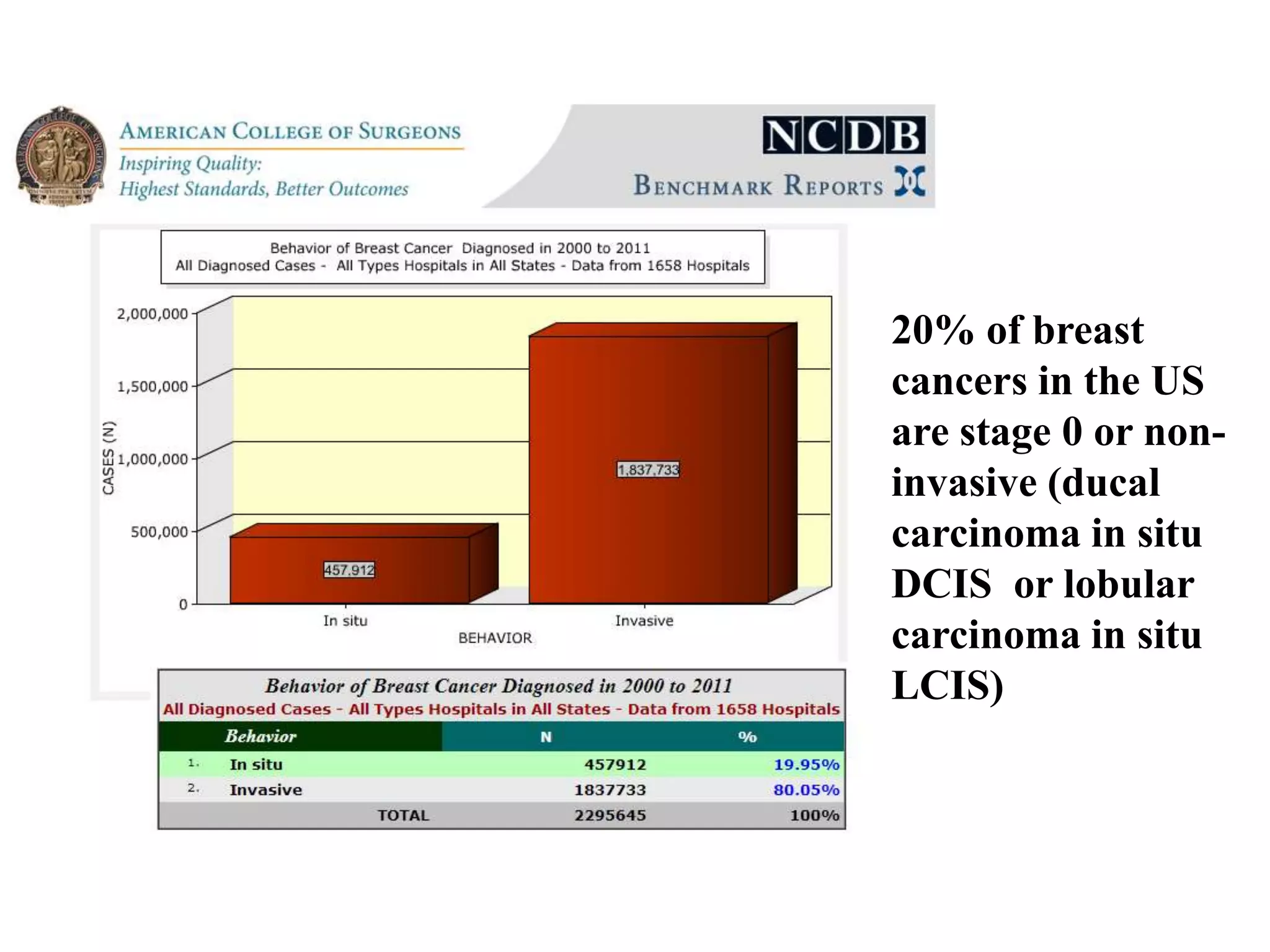

























































1) Ductal carcinoma in situ (DCIS), also known as stage 0 breast cancer, accounts for 20% of breast cancers in the US and represents the earliest non-invasive form. 2) Treatment options for DCIS include lumpectomy with or without radiation or total mastectomy. Factors such as tumor size, grade, and margin status help determine a patient's risk of recurrence and guide treatment decisions. 3) Short term side effects of breast radiation for DCIS typically include skin irritation, breast tenderness, and fatigue. Long term risks are generally low but may include lymphedema, lung inflammation, and fibrosis. Radiation reduces the risk of local recurrence by 50% compared to lumpectomy alone











































































































