Download to read offline


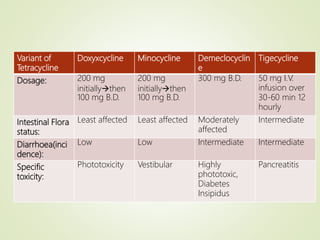

1) Tetracyclines are a class of broad-spectrum antibiotics derived from soil microorganisms. The first tetracyclines, chlortetracycline and oxytetracycline, were discovered in the 1940s-1950s. 2) Newer semi-synthetic tetracyclines like doxycycline and minocycline were developed starting in the 1950s to address problems with the older tetracyclines like resistance. 3) These newer tetracyclines have greater potency, less effect on intestinal flora, and fewer side effects compared to earlier tetracyclines.




















































































