This document discusses depression, including its epidemiology, definitions, classification, diagnostic criteria, and treatment. Some key points:
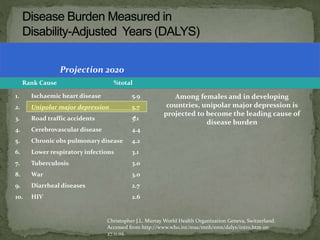
- Depression is the 3rd leading cause of disease burden worldwide and is projected to become the leading cause by 2030.
- Major depression has a prevalence of 5% and 15% of the population will experience a major depressive episode at some point in their life.
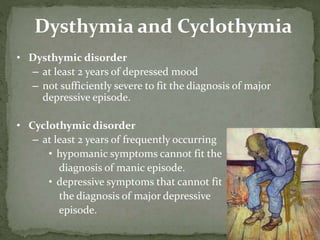
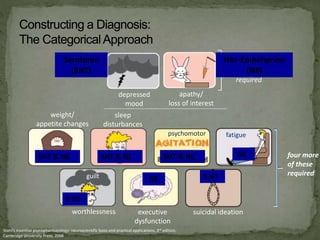
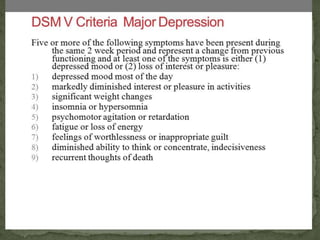
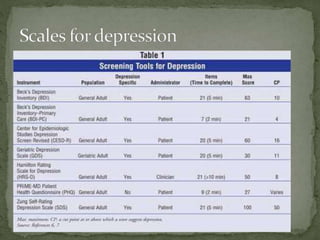
- Depression is classified based on severity from mild to severe. Diagnosis requires a certain number of symptoms from major and minor criteria groups.
- Depression can be classified as unipolar (recurrent depression only) or bipolar (episodes of mania and depression).
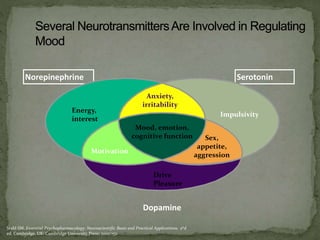
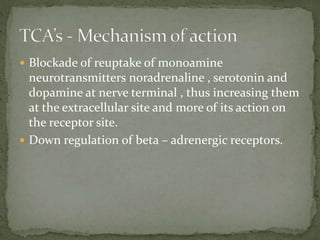
- Causes of depression involve biological factors like neurotransmitter im



















![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)

























































