Definition
• “Willis” definitionof Neoplasia - (new growth)
abnormal mass of tissue, the growth of which
exceeds and is uncoordinated with the normal
tissues and continues to grow even after the
cessation of the stimulus that evoked the
initial response
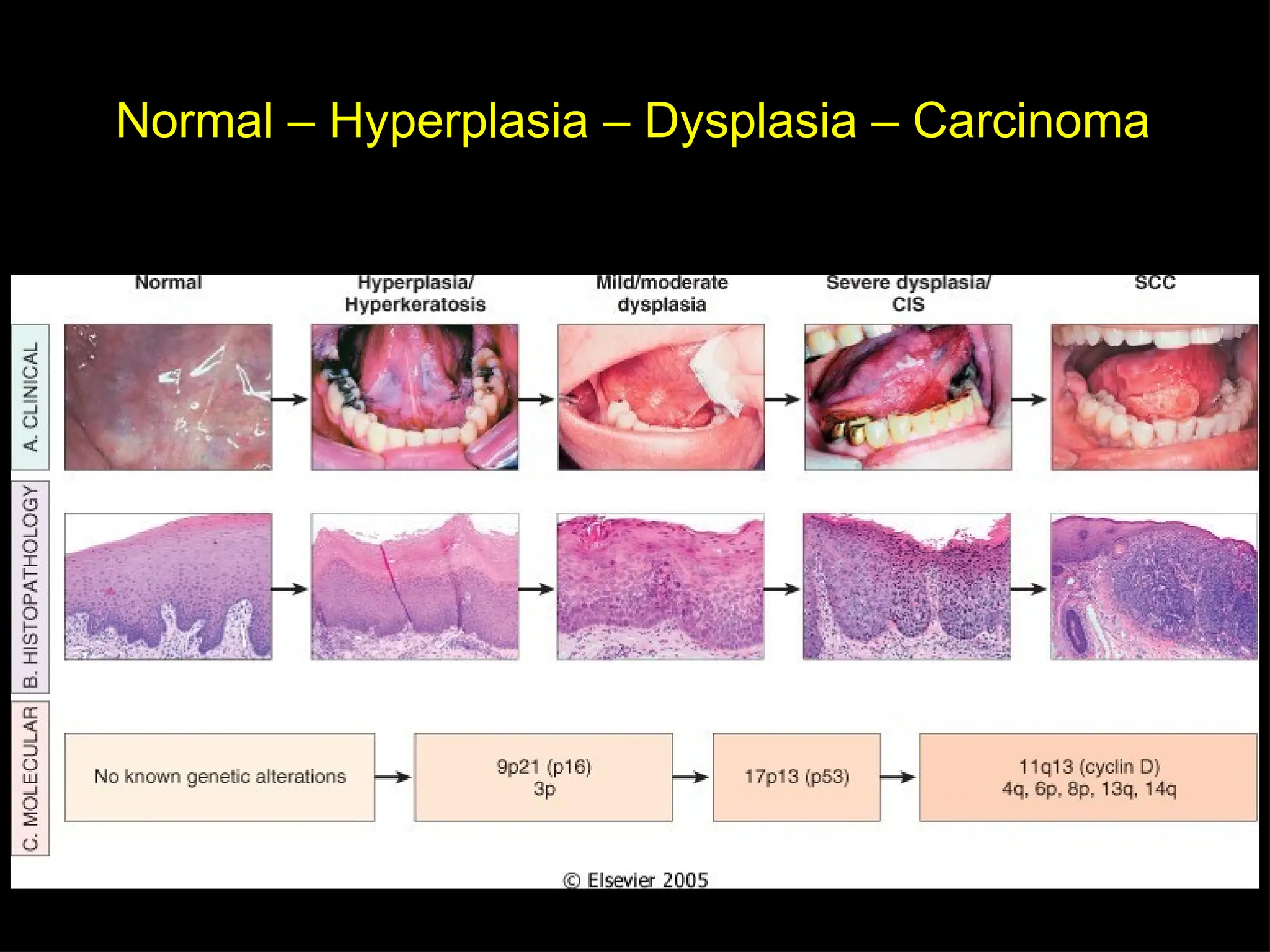
• New Definition: (Robbins Path) a neoplasm
can be defined as a disorder of cell growth
that is triggered by a series of acquired
mutations affecting a single cell and its clonal
progeny
Neoplasm
The causative mutationsgive the
neoplastic cells a survival and growth
advantage, resulting in excessive
proliferation that is independent
of physiologic growth signals
(autonomous)
27.
Neoplasia
• It isautonomous, purposeless
• Proliferation is uncontrolled
• Competes with normal cells for its needs
• It is a clonal disorder
• It is a genetic disorder
– In 95% of cases acquired genetic disorder
– In 5% of cases inherited
28.
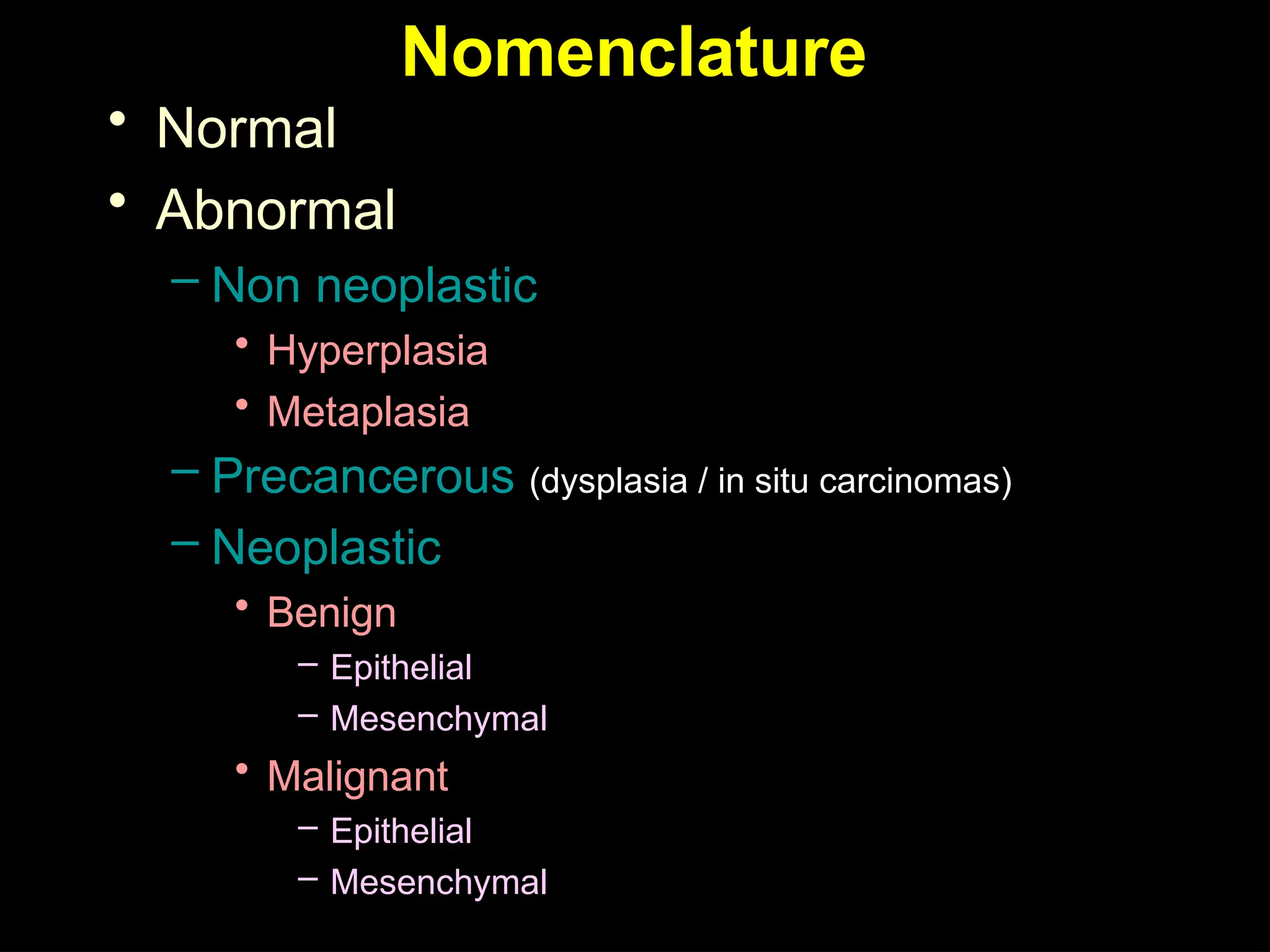
Nomenclature
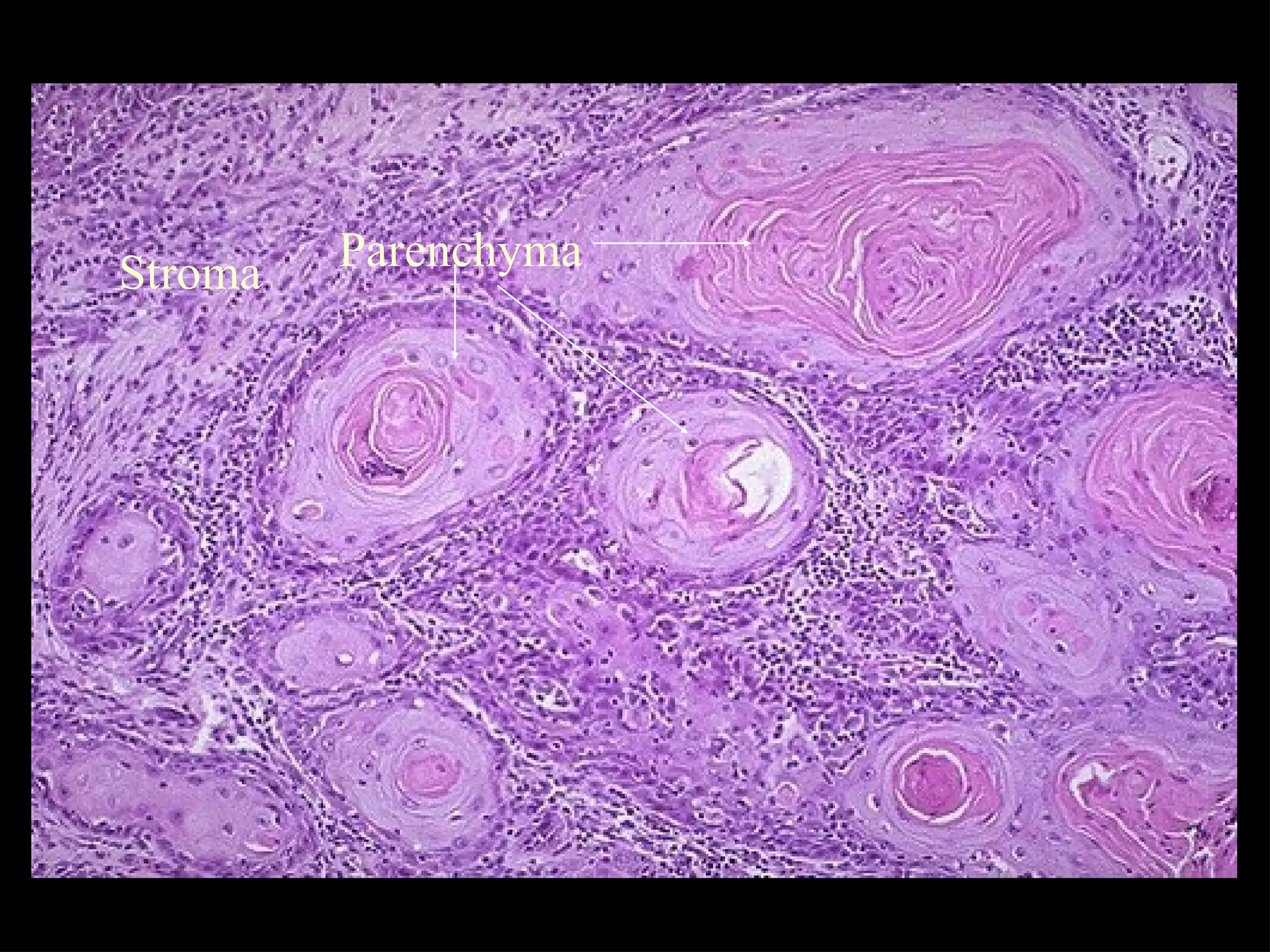
• All tumorshave two components
– Parenchyma
• Represents tumor proper; the growth of the tumor
is due to proliferation of these cells
– Stroma
• Provides the framework, blood supply and nutrition
for the parenchymal cells
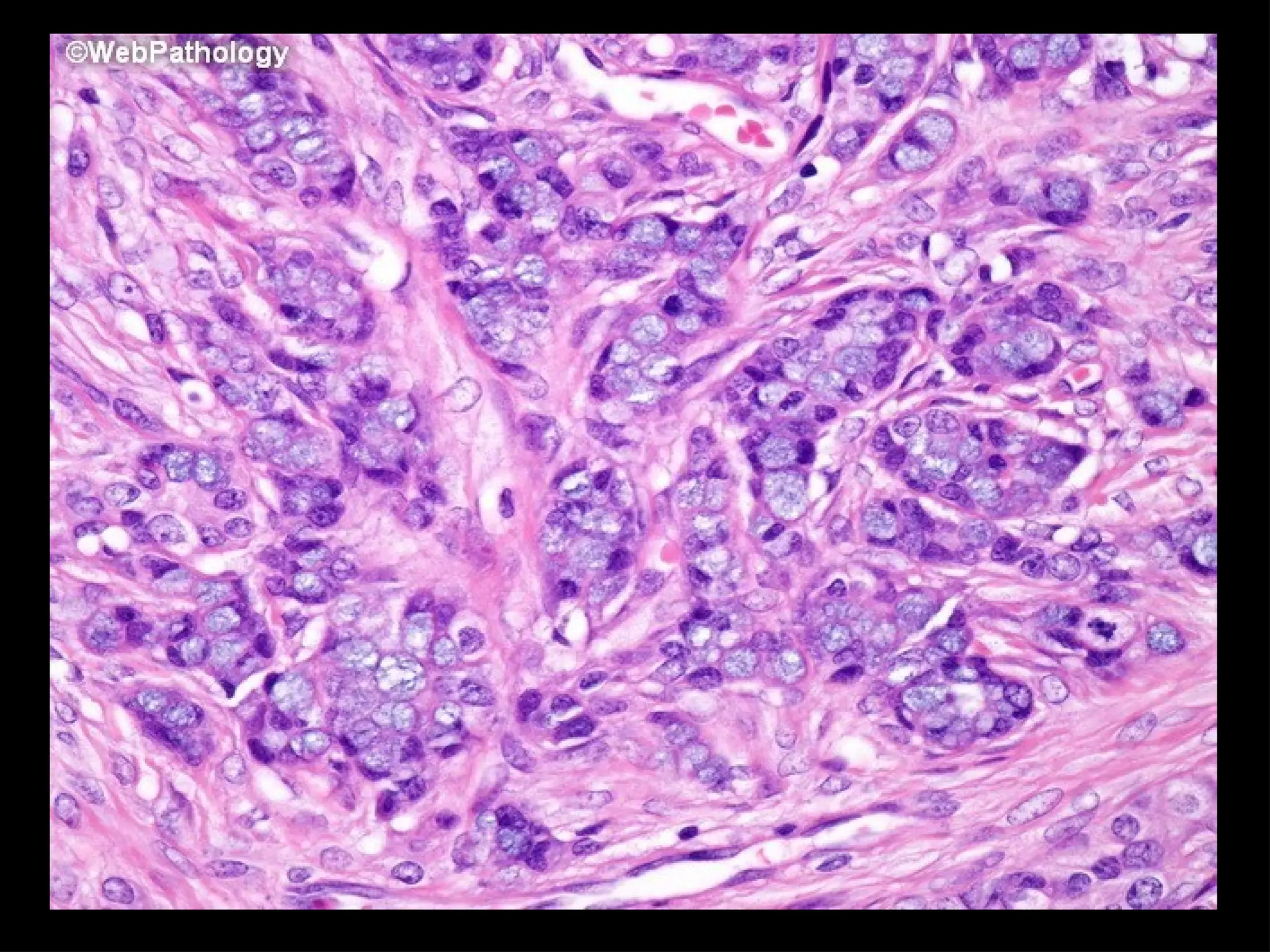
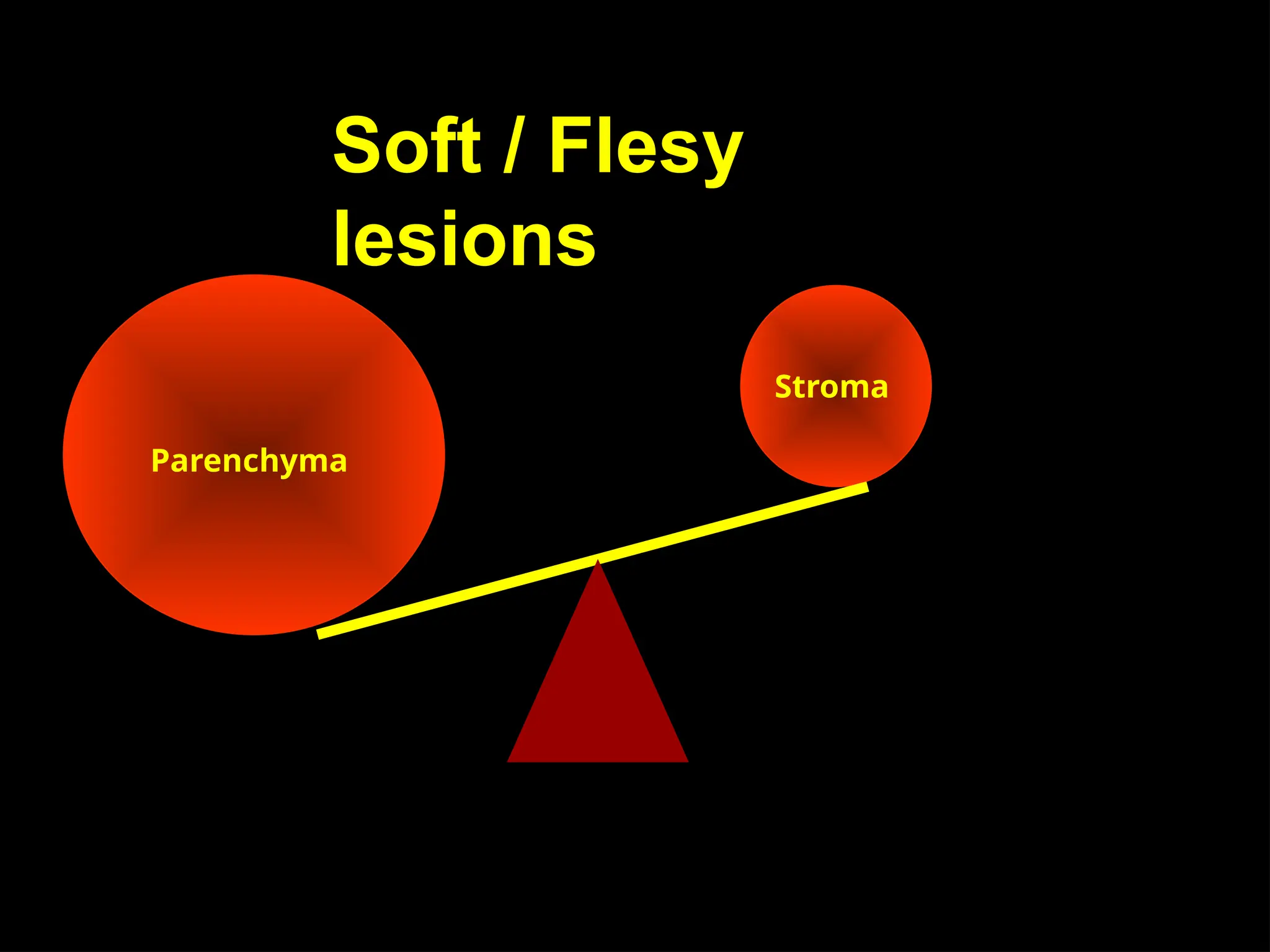
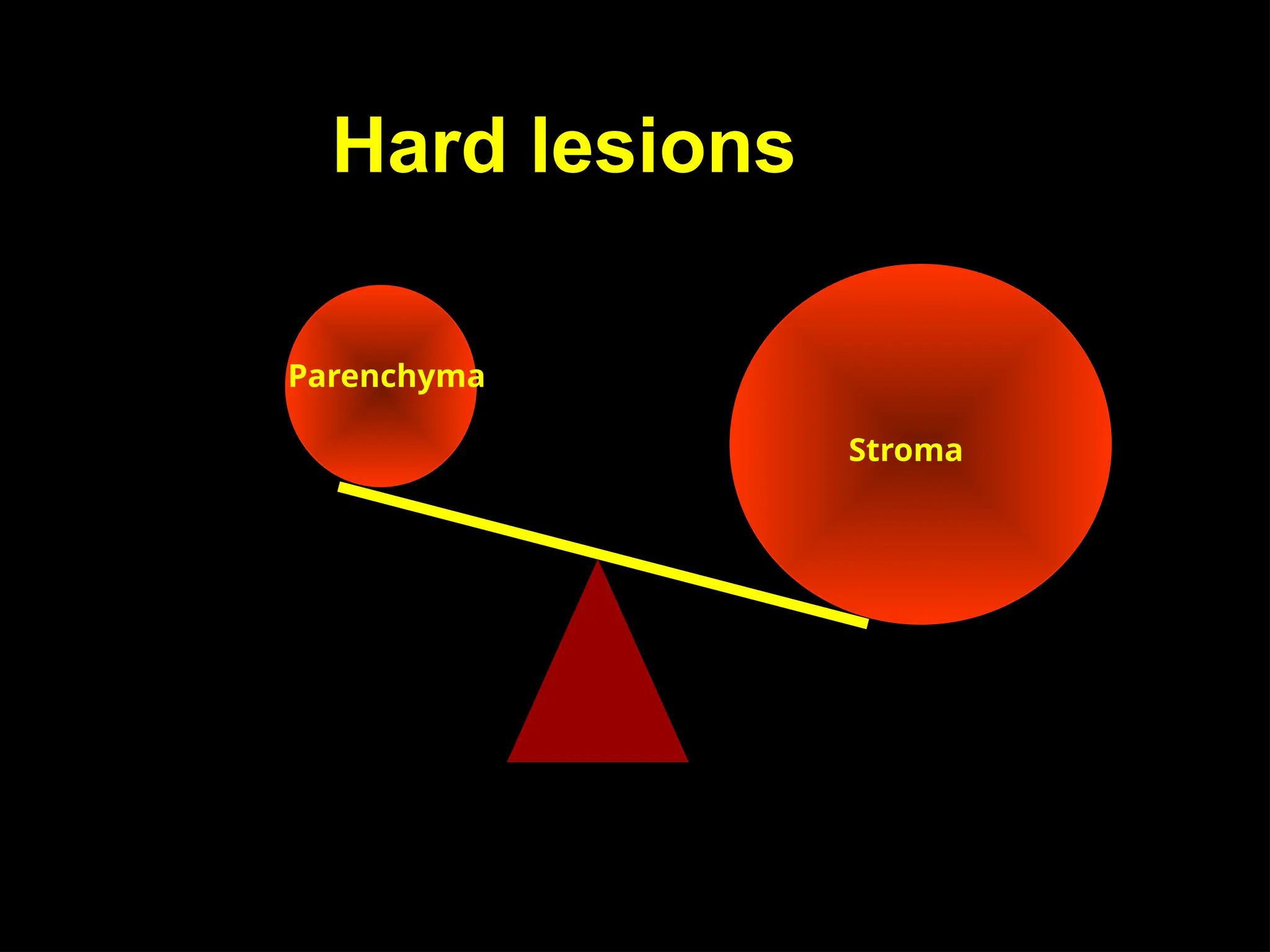
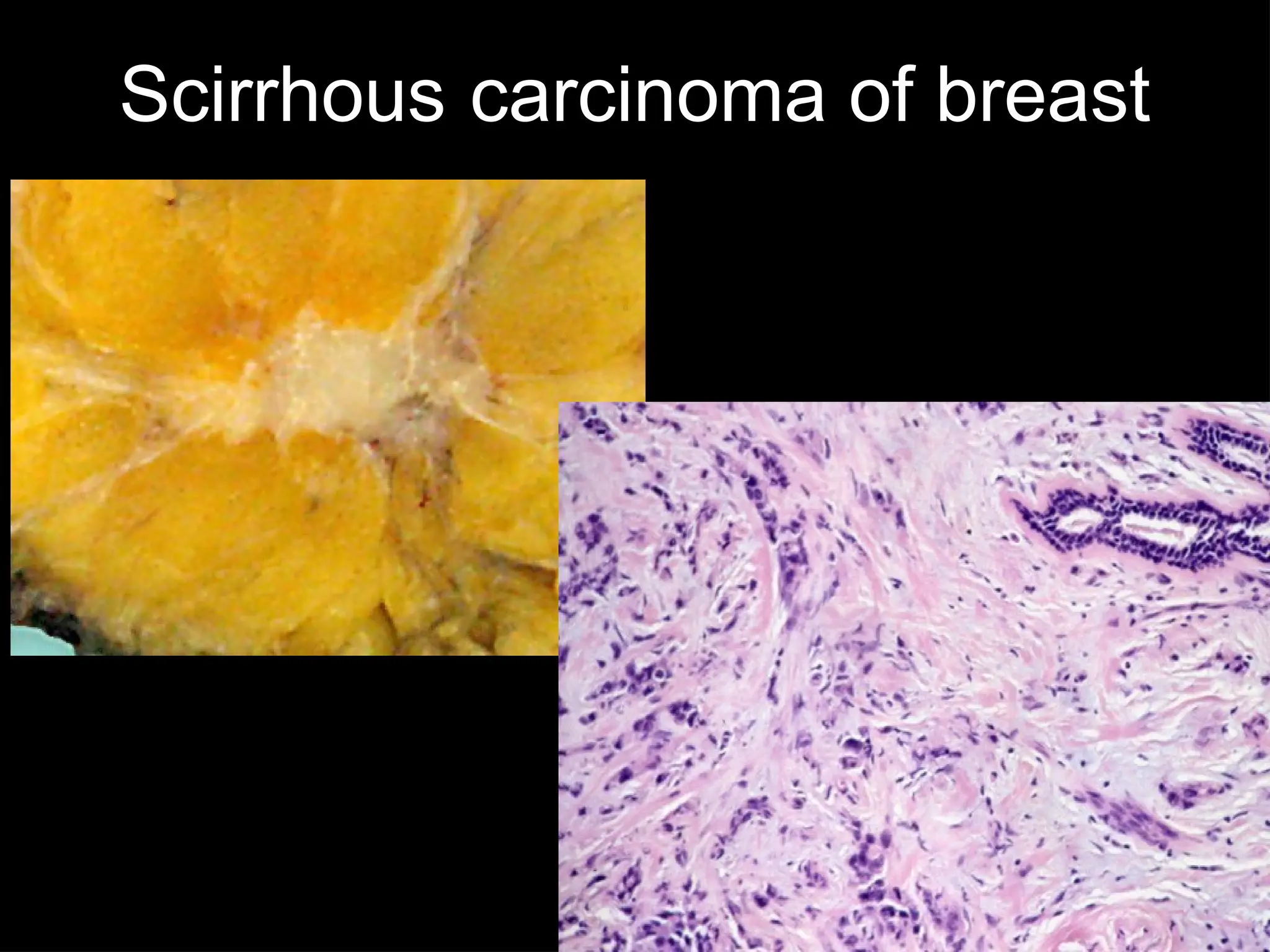
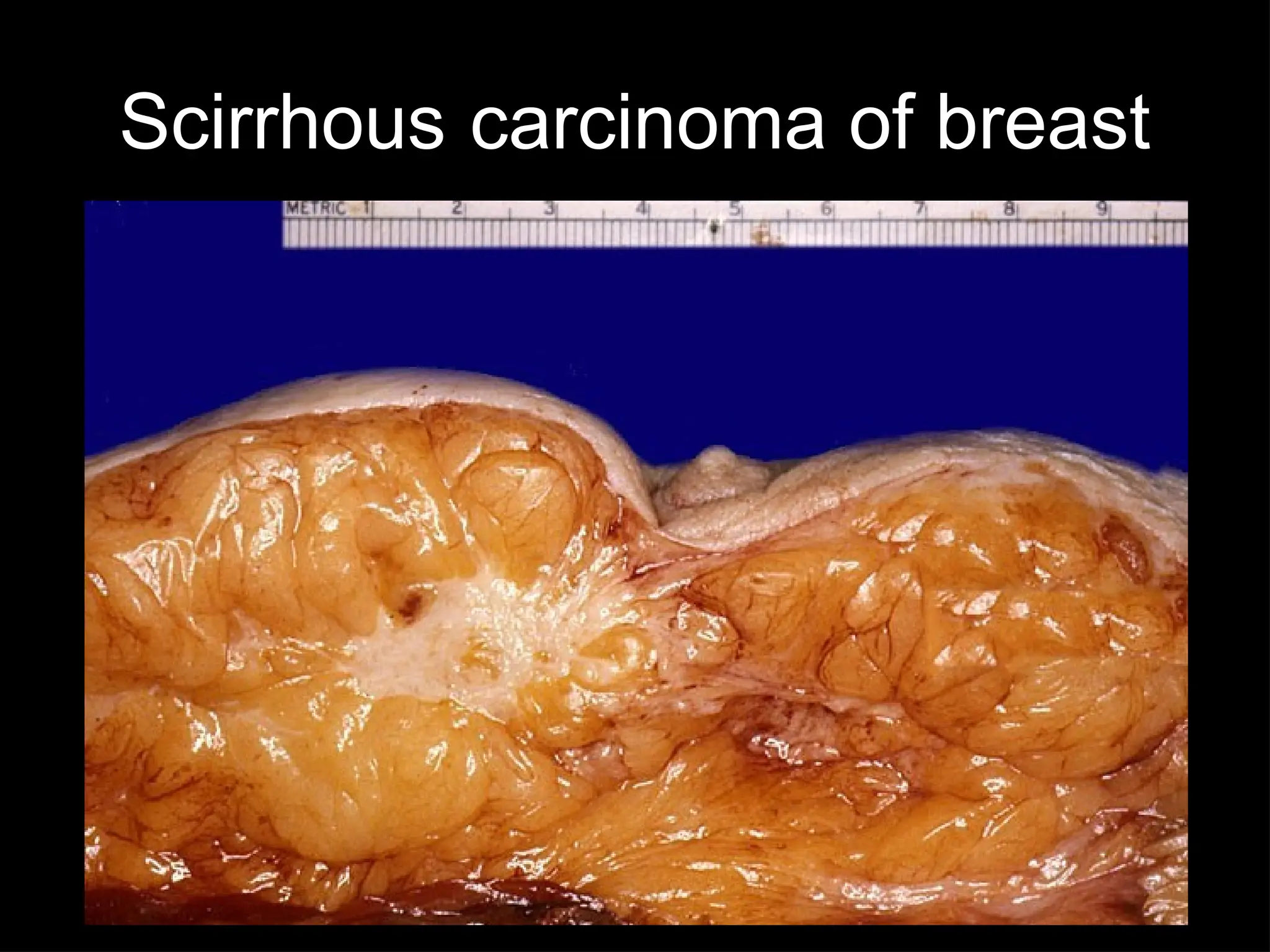
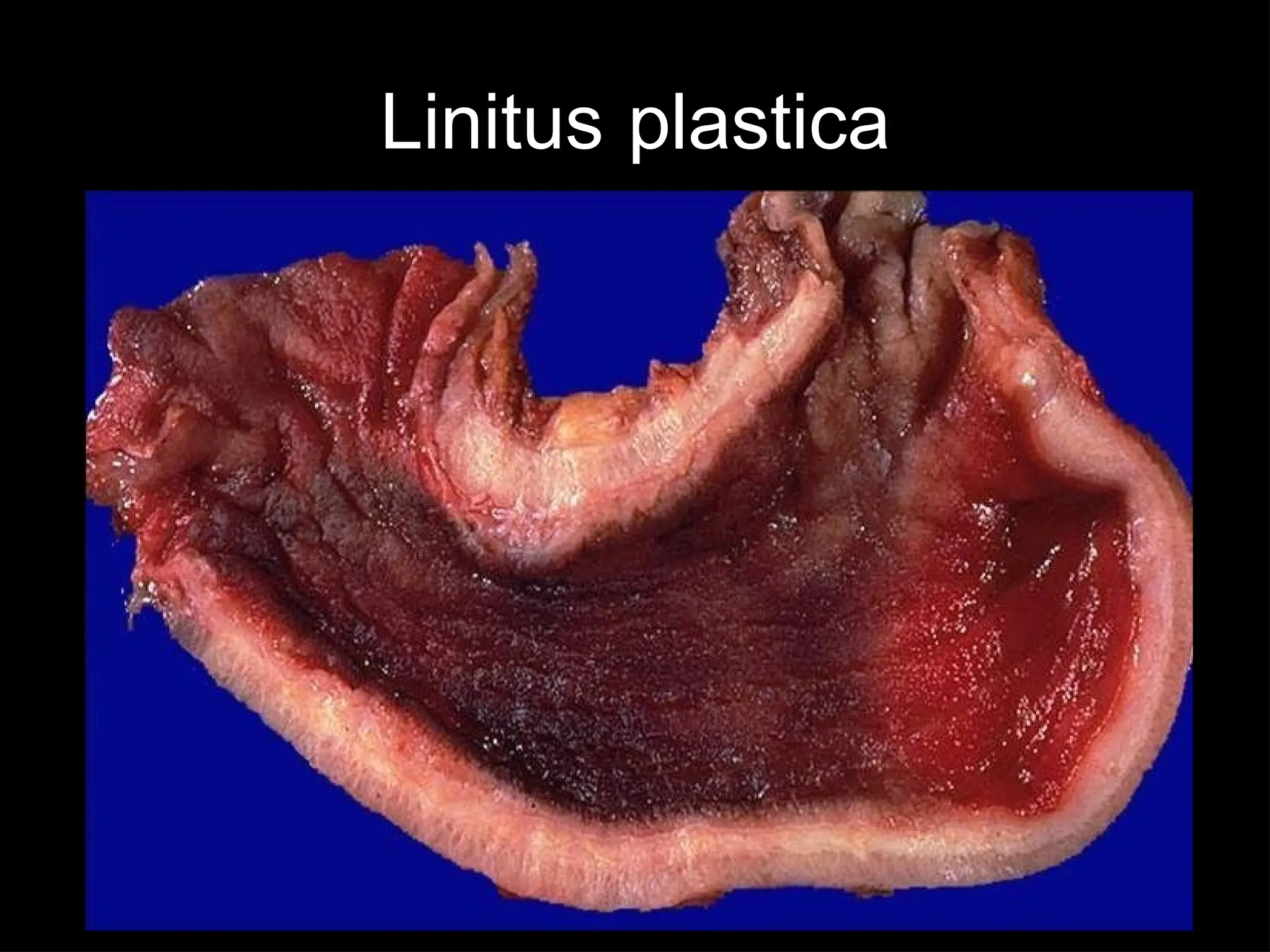
Desmoplasia
• Formation ofabundant collagenous stroma
• Stimulated by parenchymal cells
• Ex: Schirrous. ca of breast
Linitus plastica (ca stomach)
Carcinoma prostate
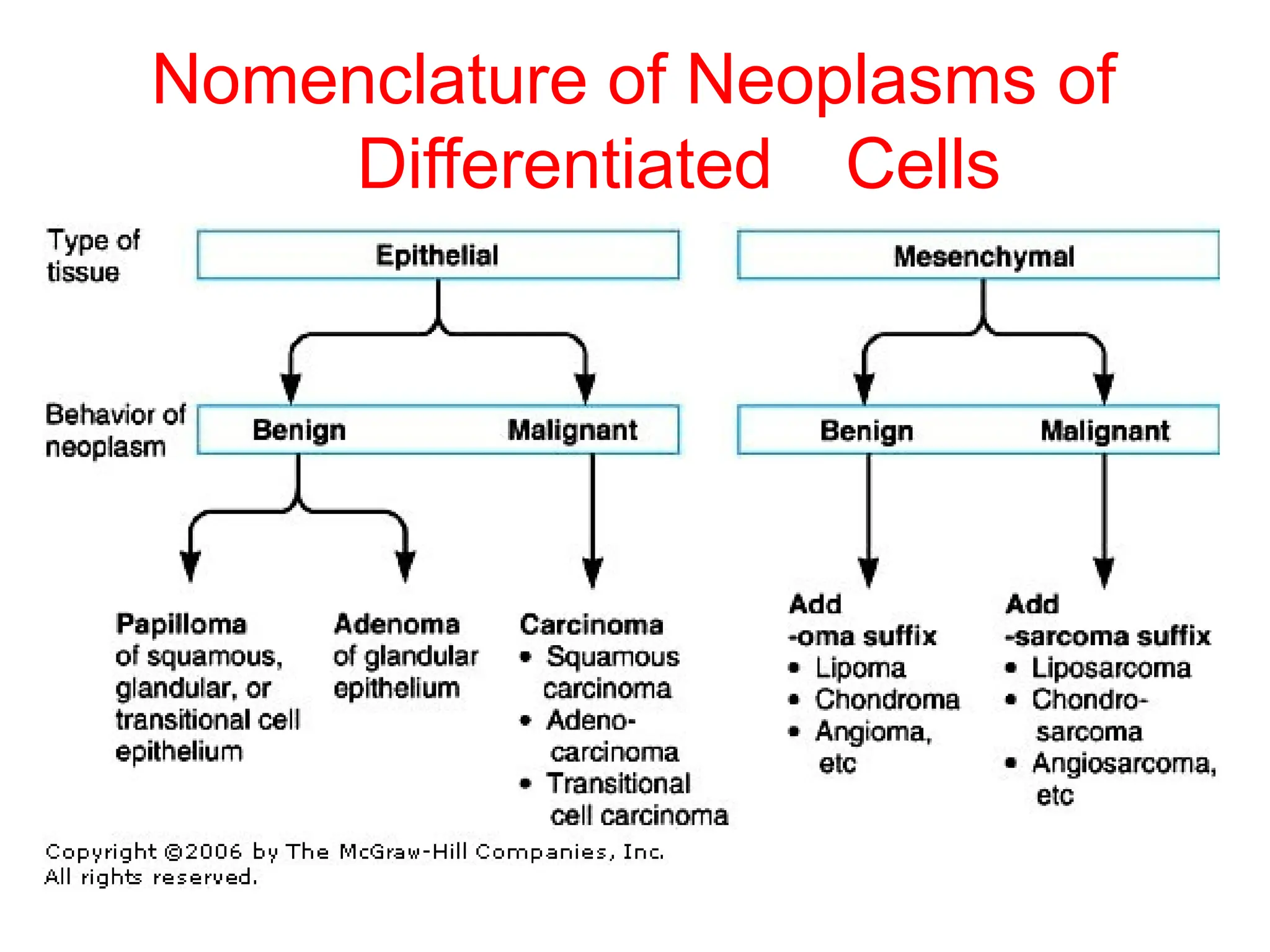
Nomenclature
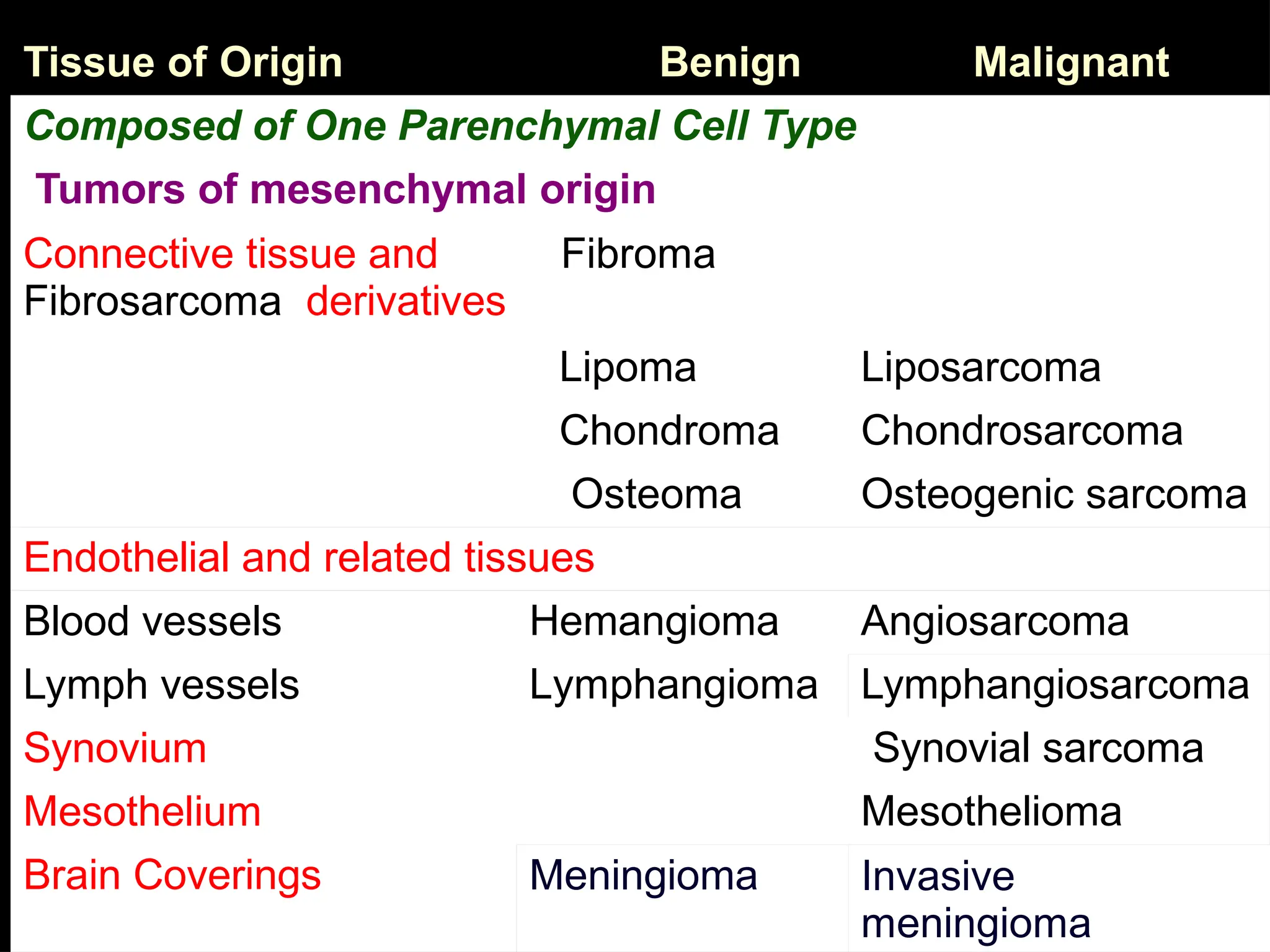
• Tumors aredesignated by attaching suffix “–oma”
to the cell or tissue of origin
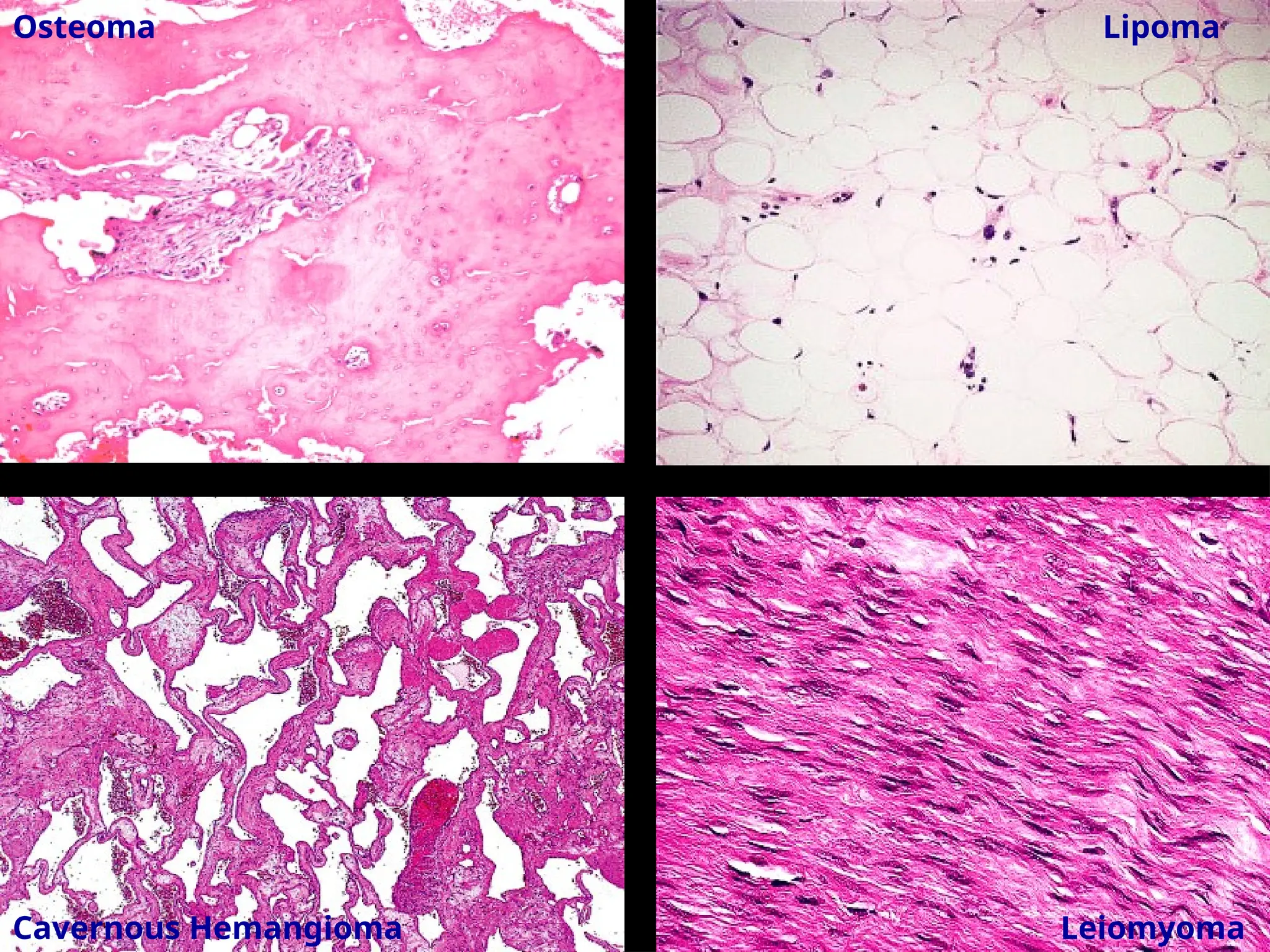
– Fibroma, chondroma, lipoma, osteoma etc
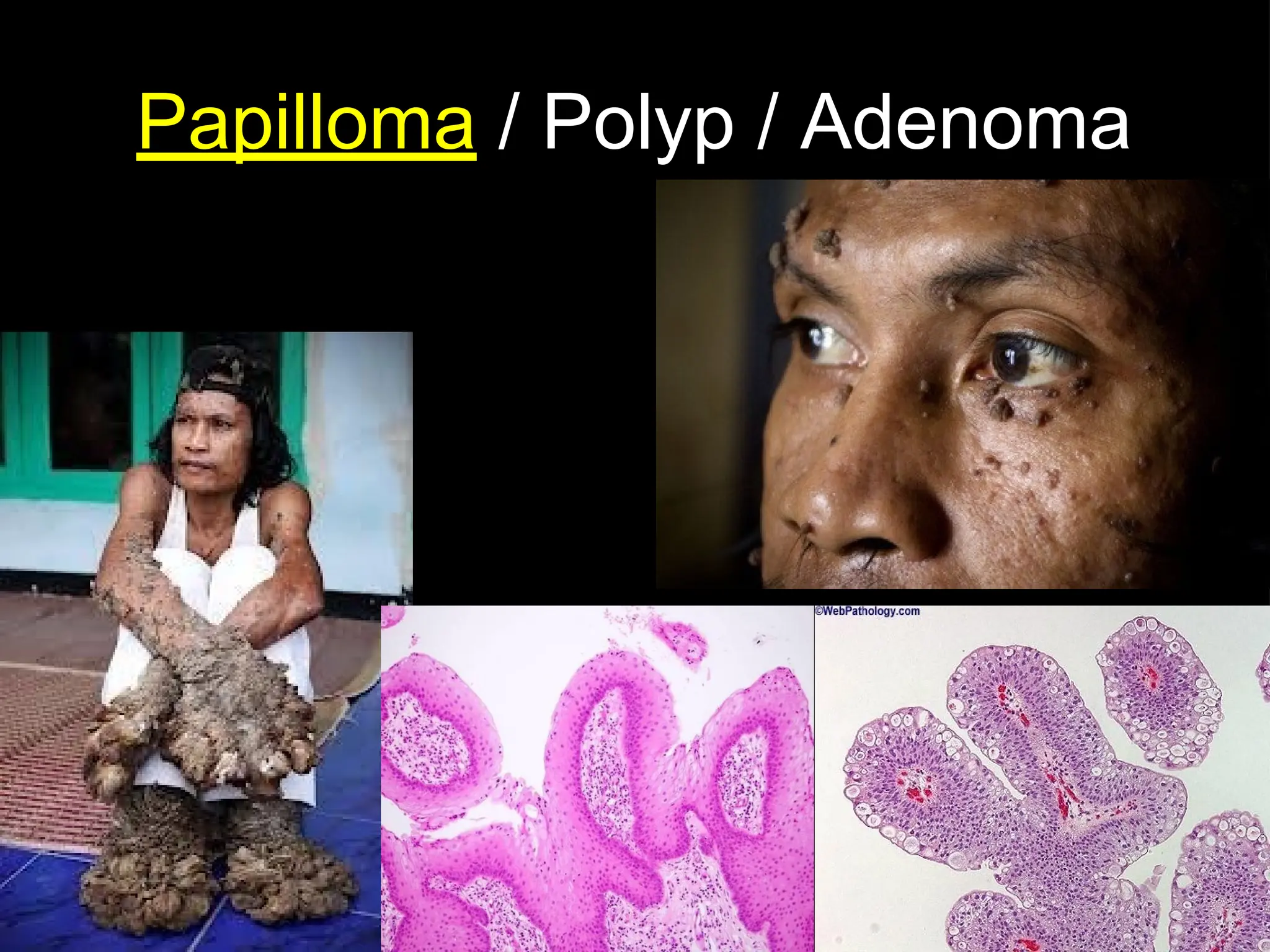
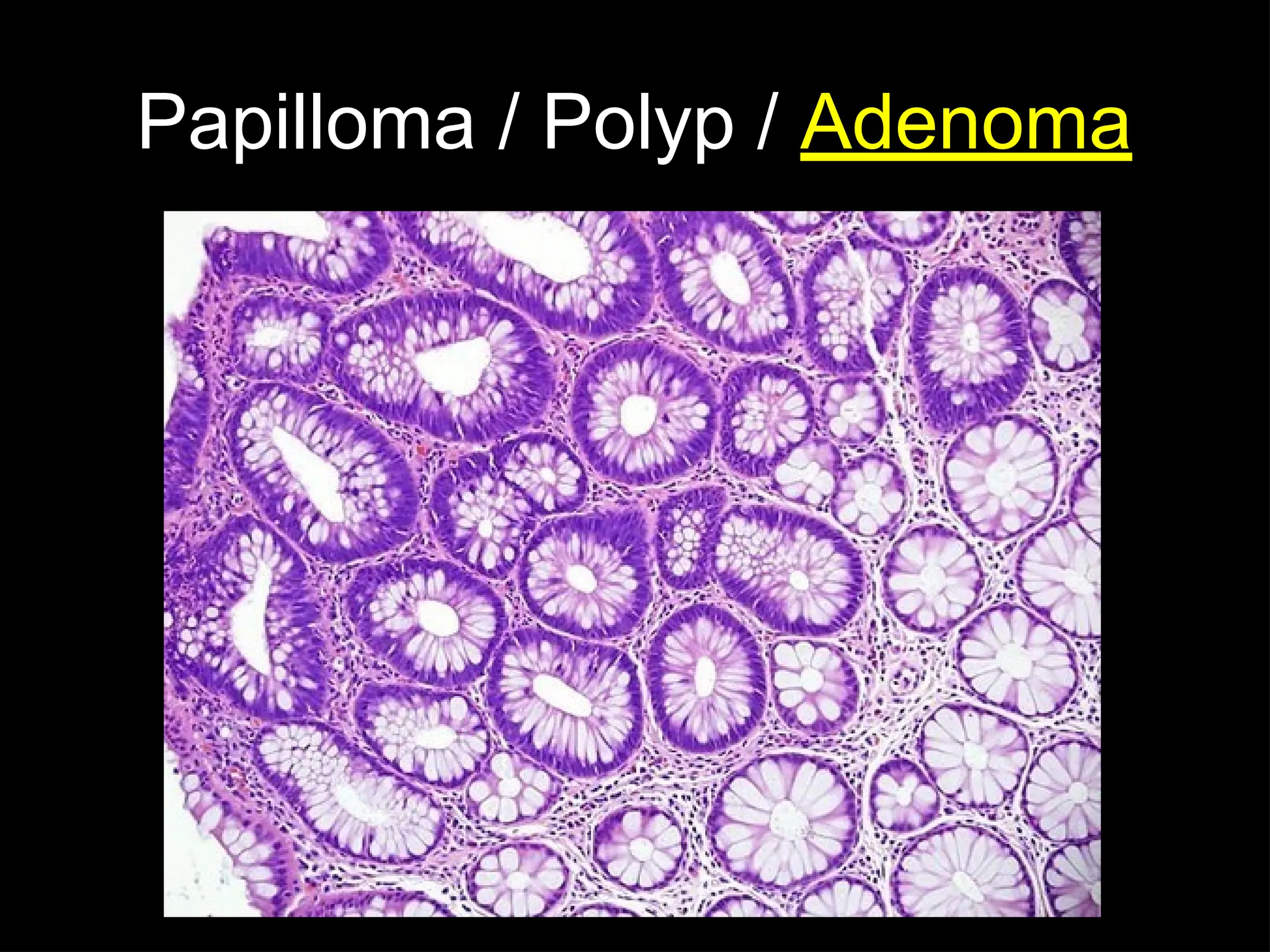
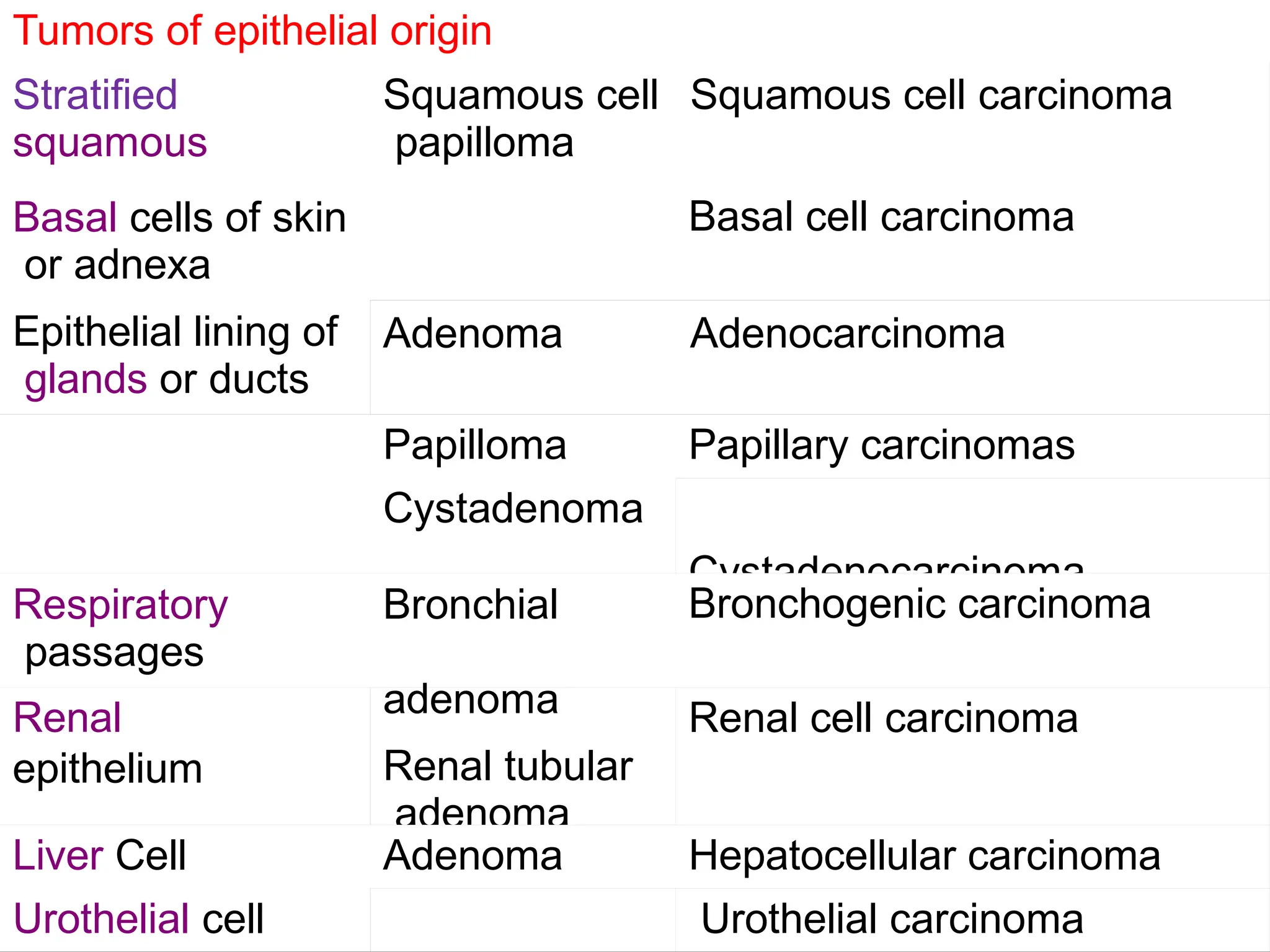
– Benign tumor arising from glandular structure is called
adenoma
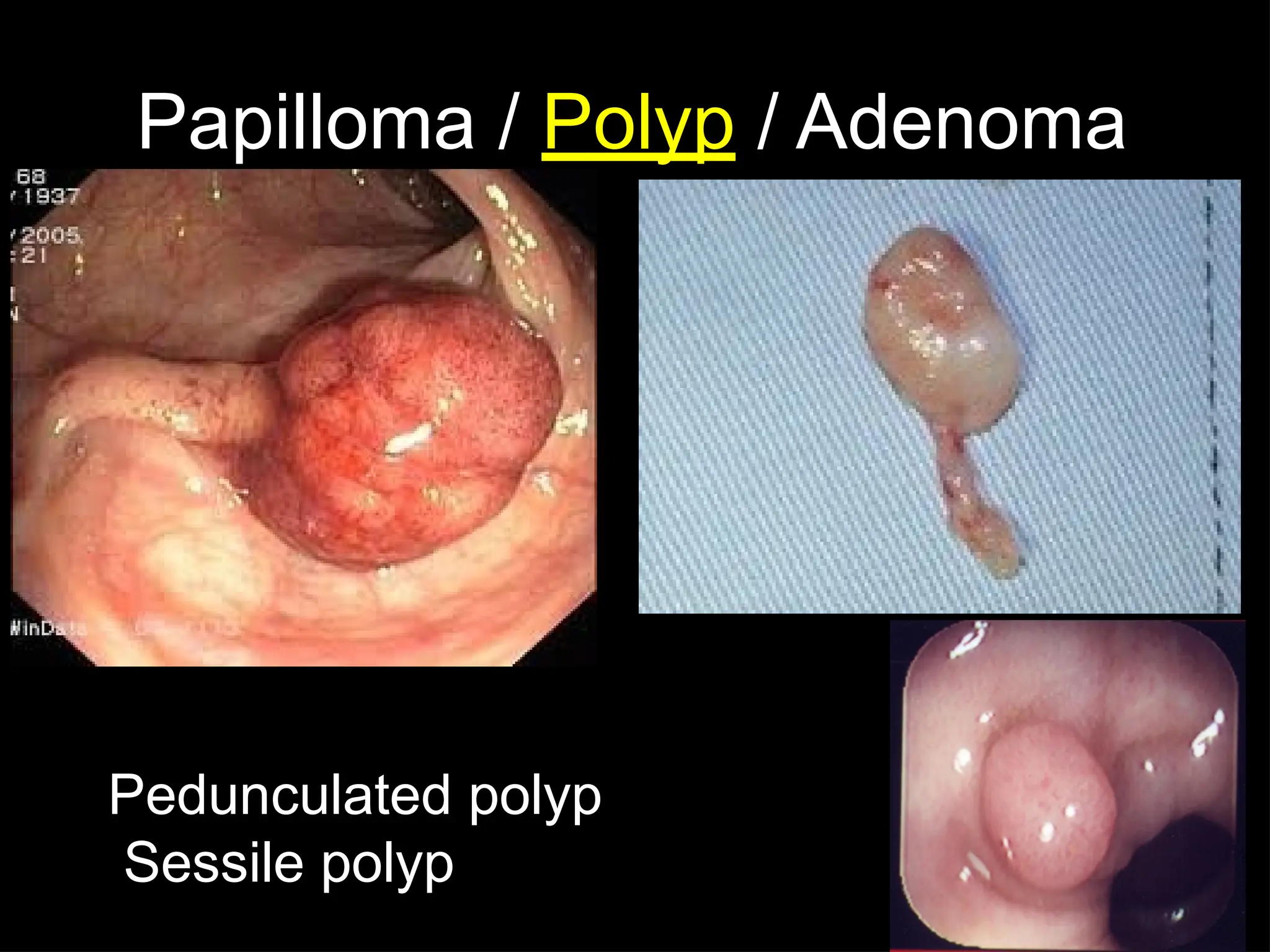
– Benign tumor arising from epithelial surface having finger
like projections is called papilloma
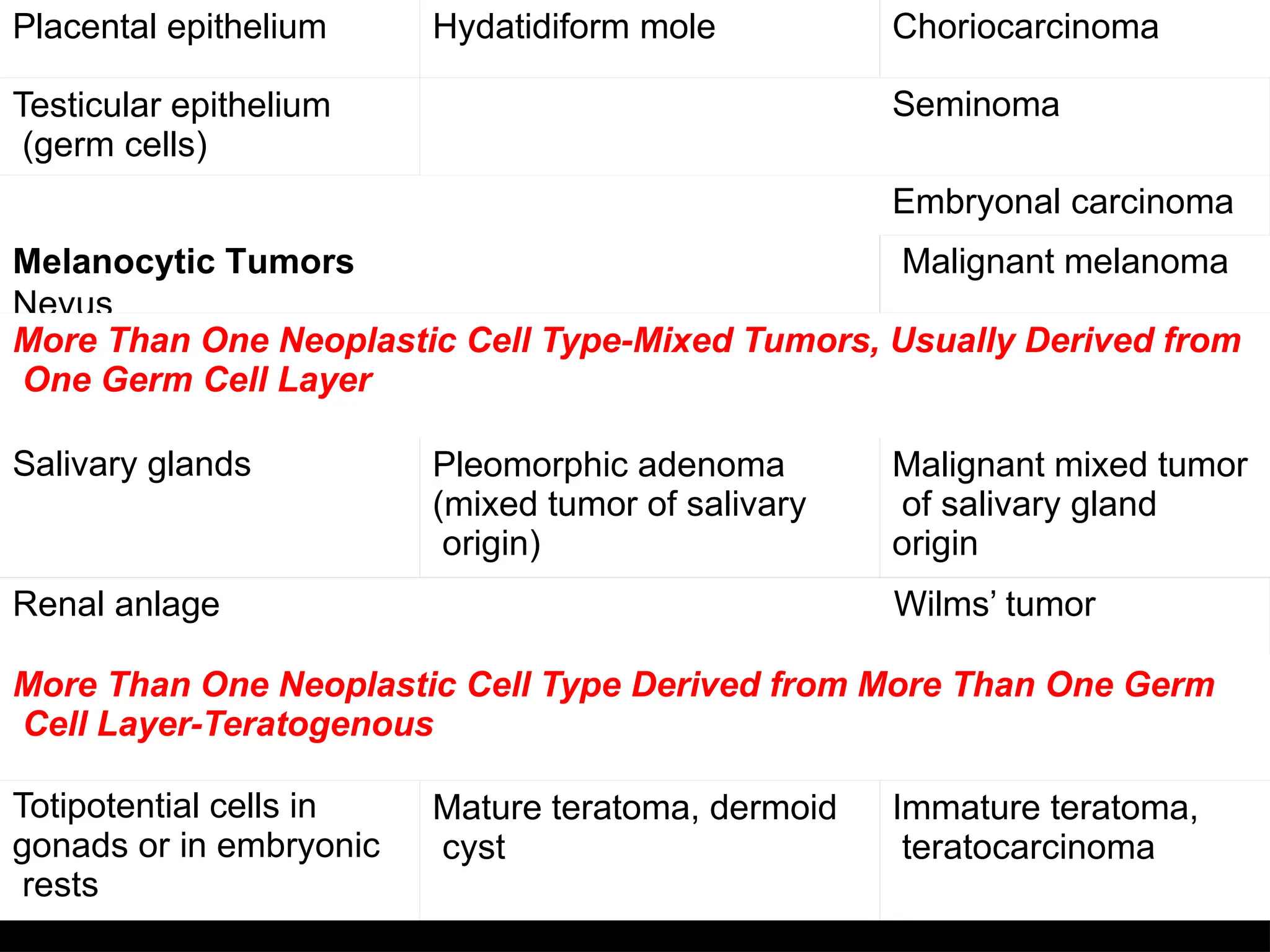
Placental epithelium Hydatidiformmole Choriocarcinoma
Testicular epithelium
(germ cells)
Seminoma
Melanocytic Tumors
Nevus
Embryonal carcinoma
Malignant melanoma
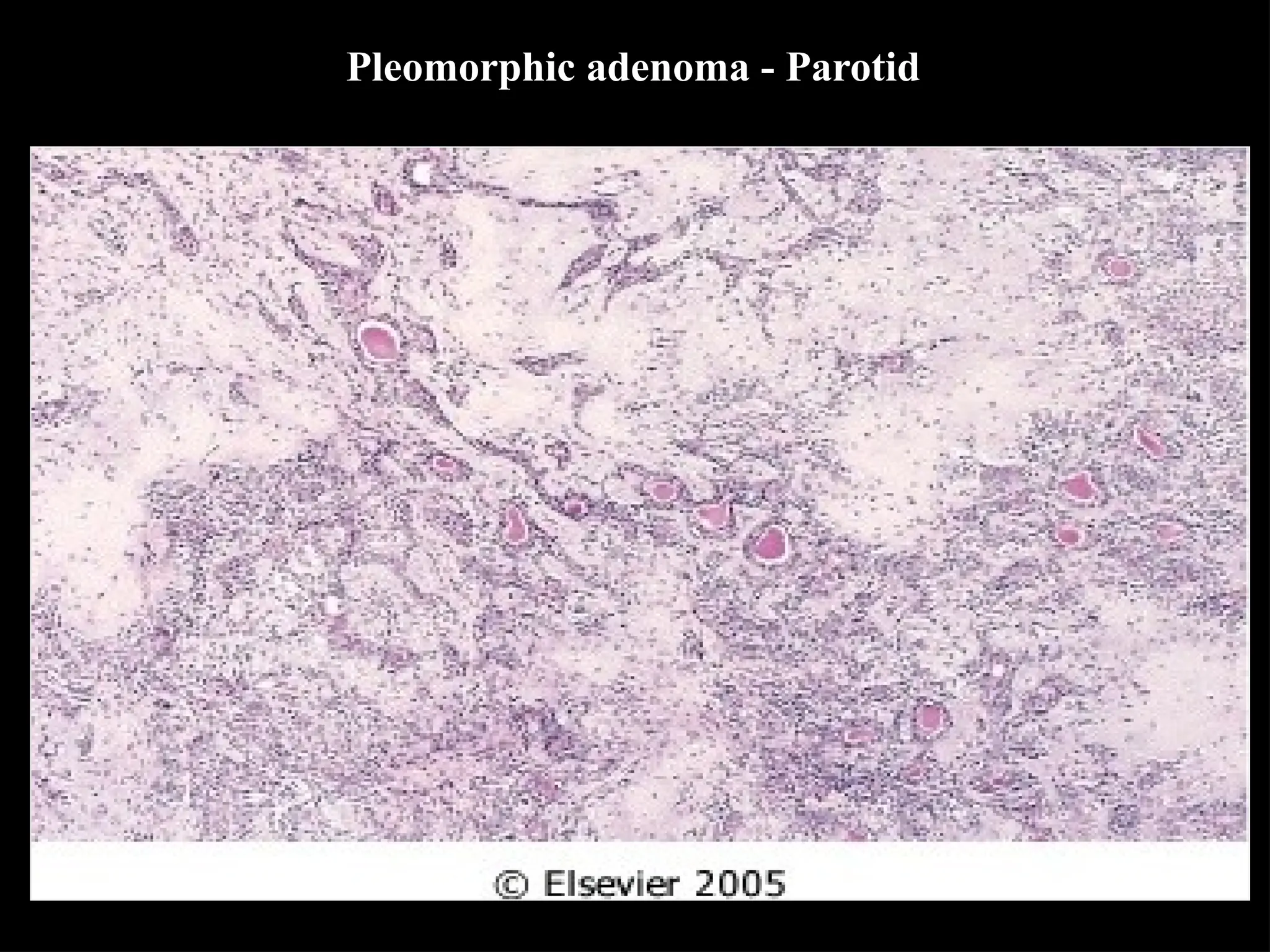
More Than One Neoplastic Cell Type-Mixed Tumors, Usually Derived from
One Germ Cell Layer
Salivary glands Pleomorphic adenoma
(mixed tumor of salivary
origin)
Malignant mixed tumor
of salivary gland
origin
Renal anlage Wilms’ tumor
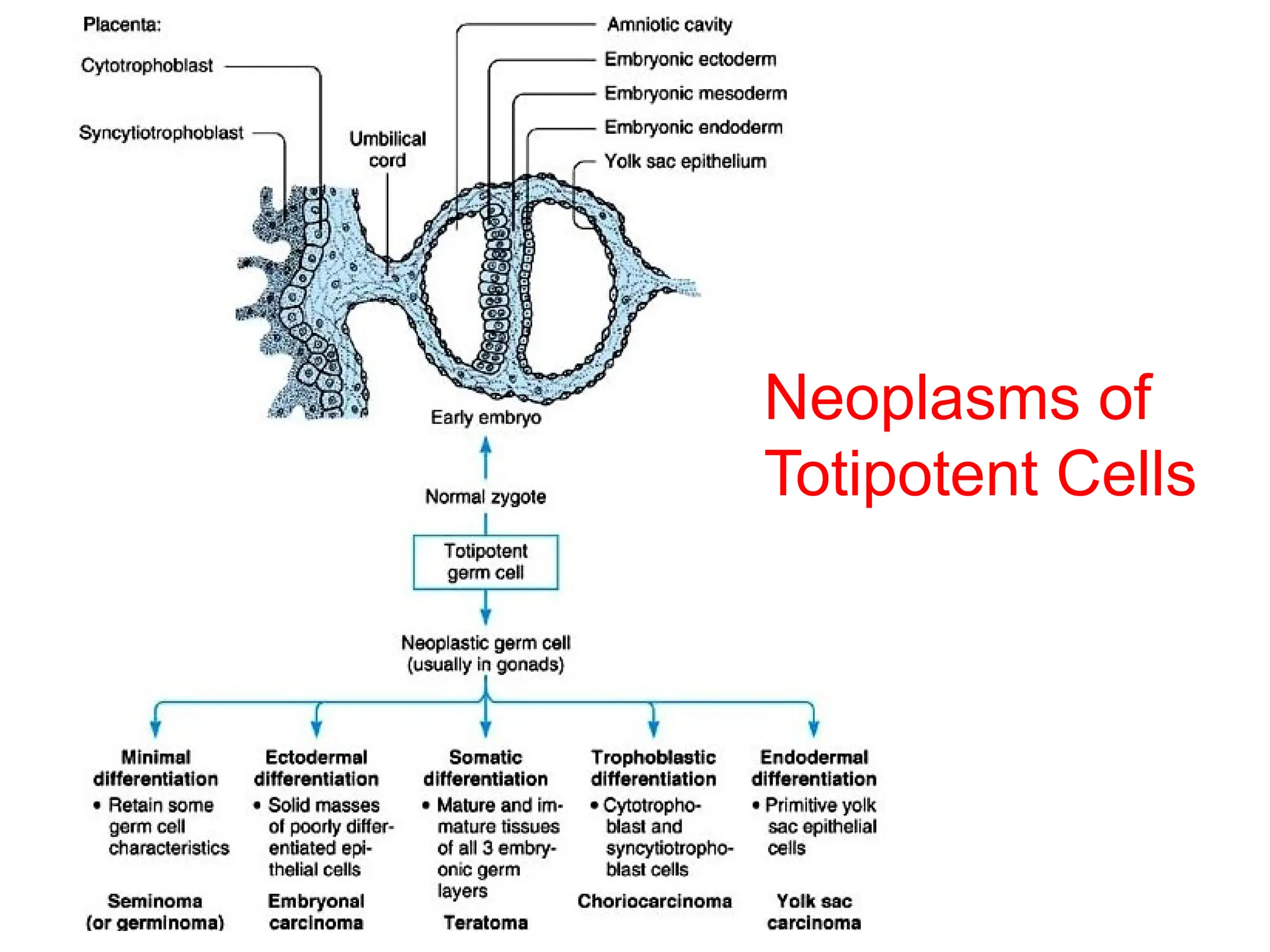
More Than One Neoplastic Cell Type Derived from More Than One Germ
Cell Layer-Teratogenous
Totipotential cells in
gonads or in embryonic
rests
Mature teratoma, dermoid
cyst
Immature teratoma,
teratocarcinoma
46.
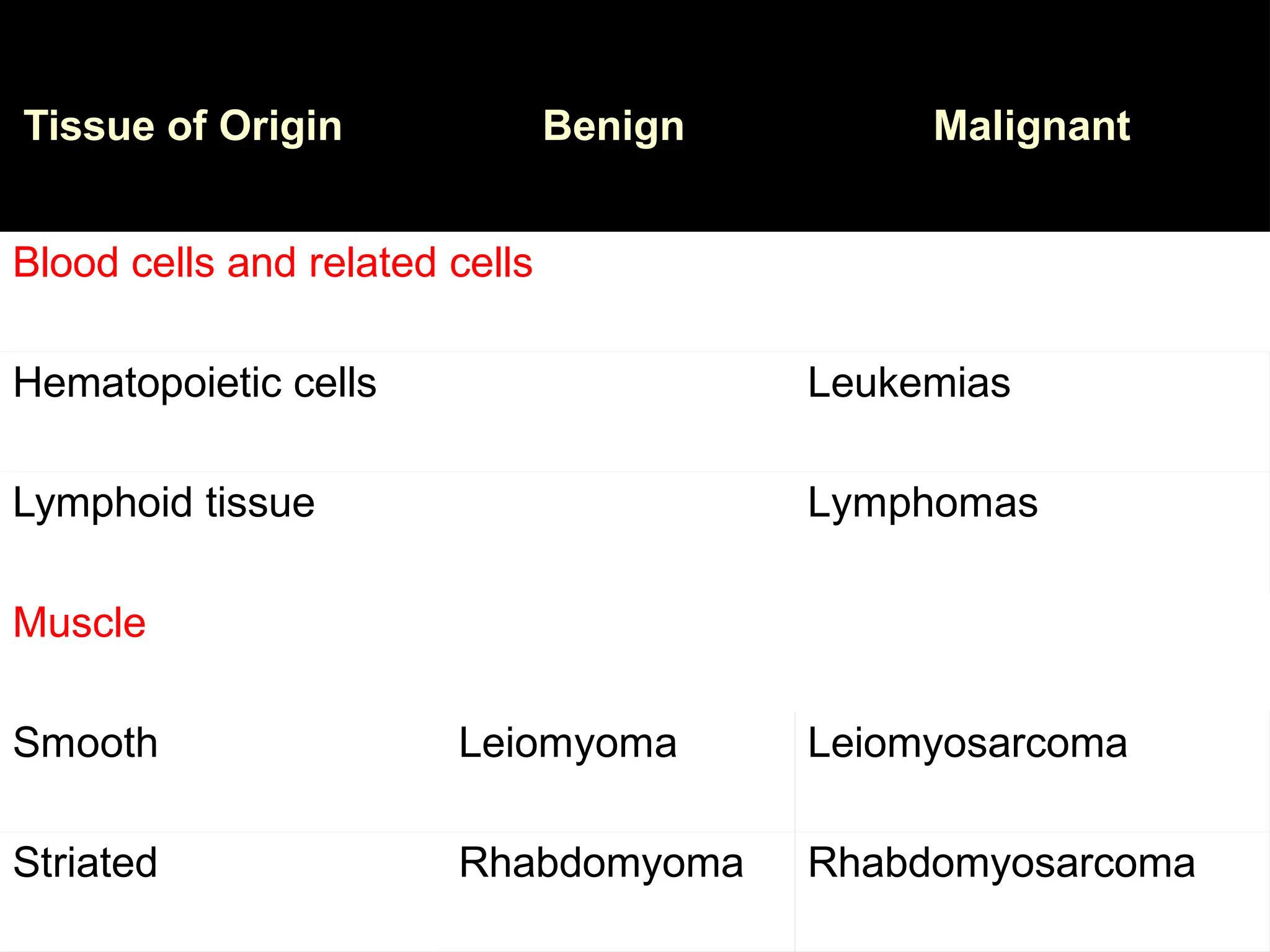
Tissues with NObenign tumors
• Synovium
• Mesothelium
• Lymphoid tissue
• Hematopoietic cells
• Basal cells of skin or adnexa
47.
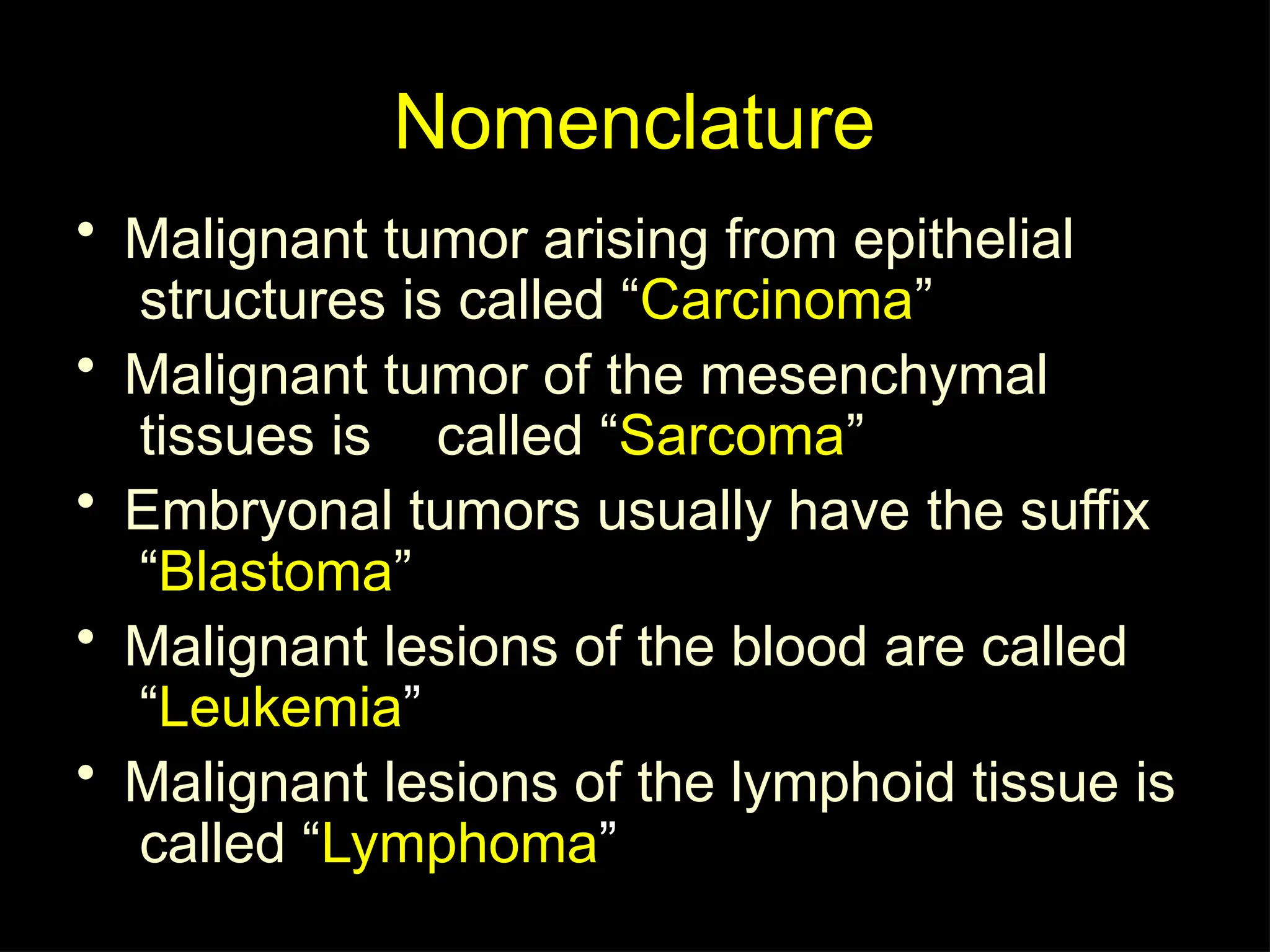
Nomenclature
• Malignant tumorarising from epithelial
structures is called “Carcinoma”
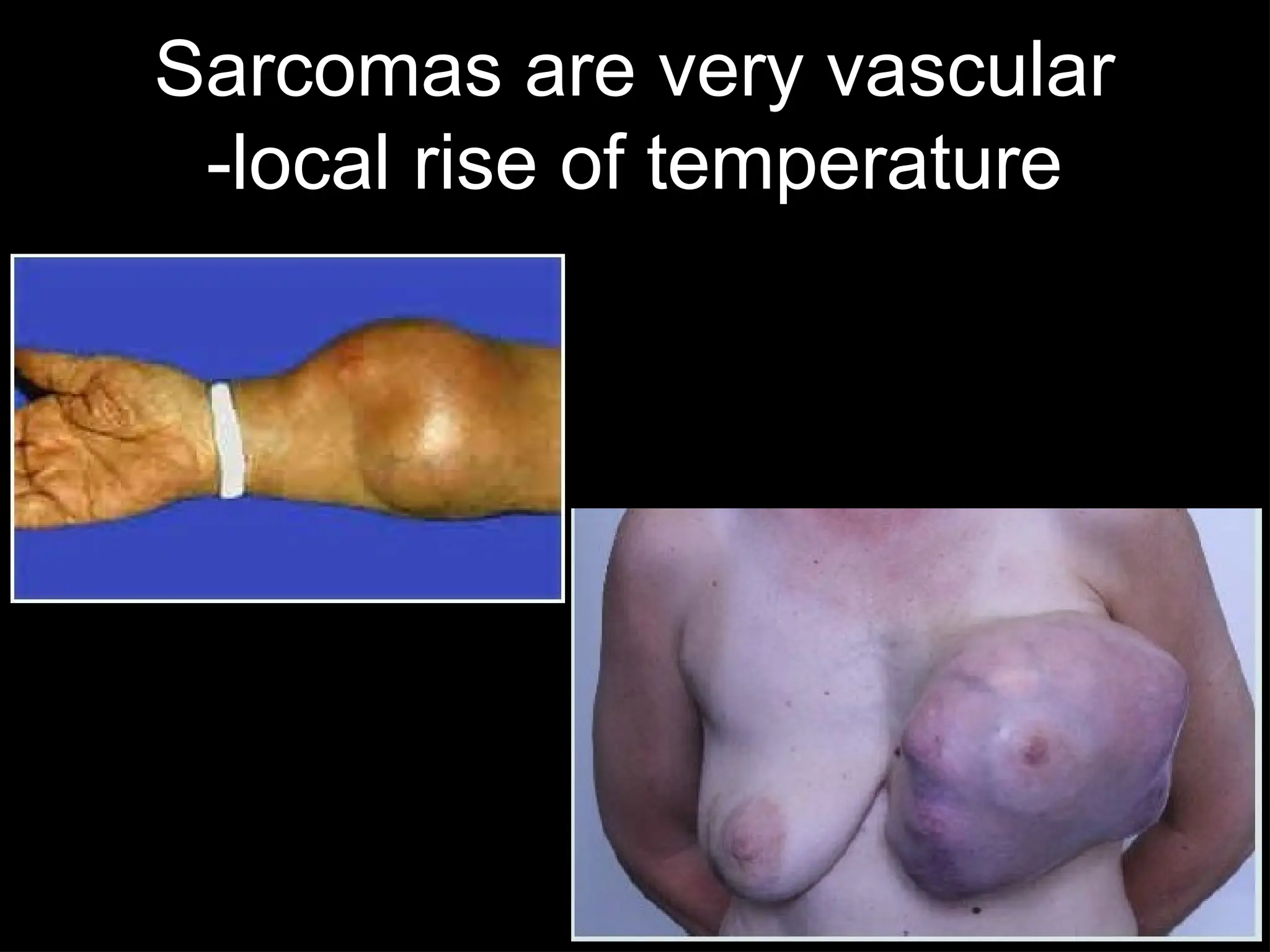
• Malignant tumor of the mesenchymal
tissues is called “Sarcoma”
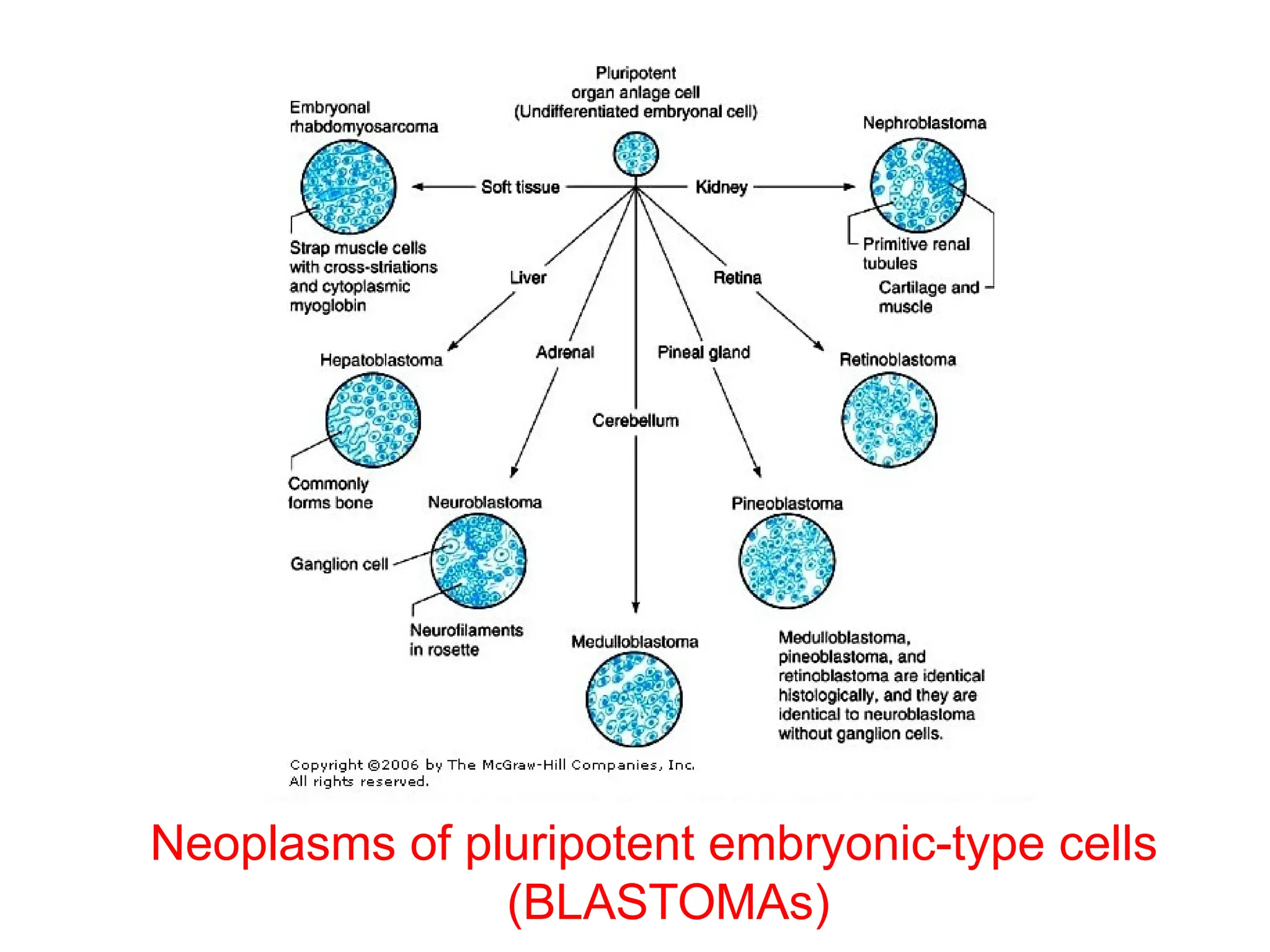
• Embryonal tumors usually have the suffix
“Blastoma”
• Malignant lesions of the blood are called
“Leukemia”
• Malignant lesions of the lymphoid tissue is
called “Lymphoma”
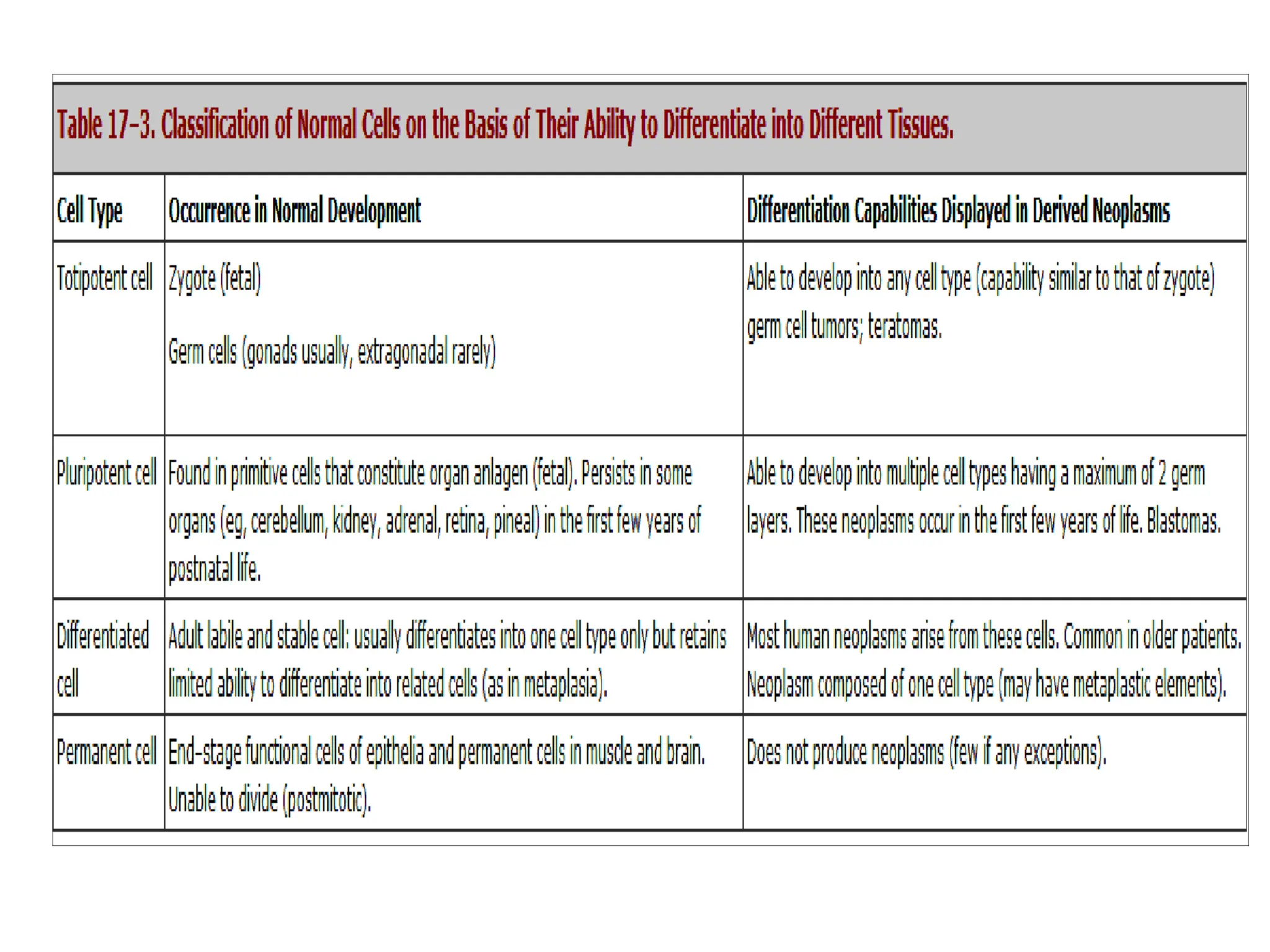
Neoplasms of Embryonic
PluripotentCells
• Pluripotent cells can mature into several
different cell types
• These neoplasms are generally called
Embryomas or Blastomas
51.
Blastoma
• All blastomasare childhood tumors
• All blastomas are malignant tumors
Except:
–Chondroblastoma
–Osteoblastoma
–Pulmonary blastoma
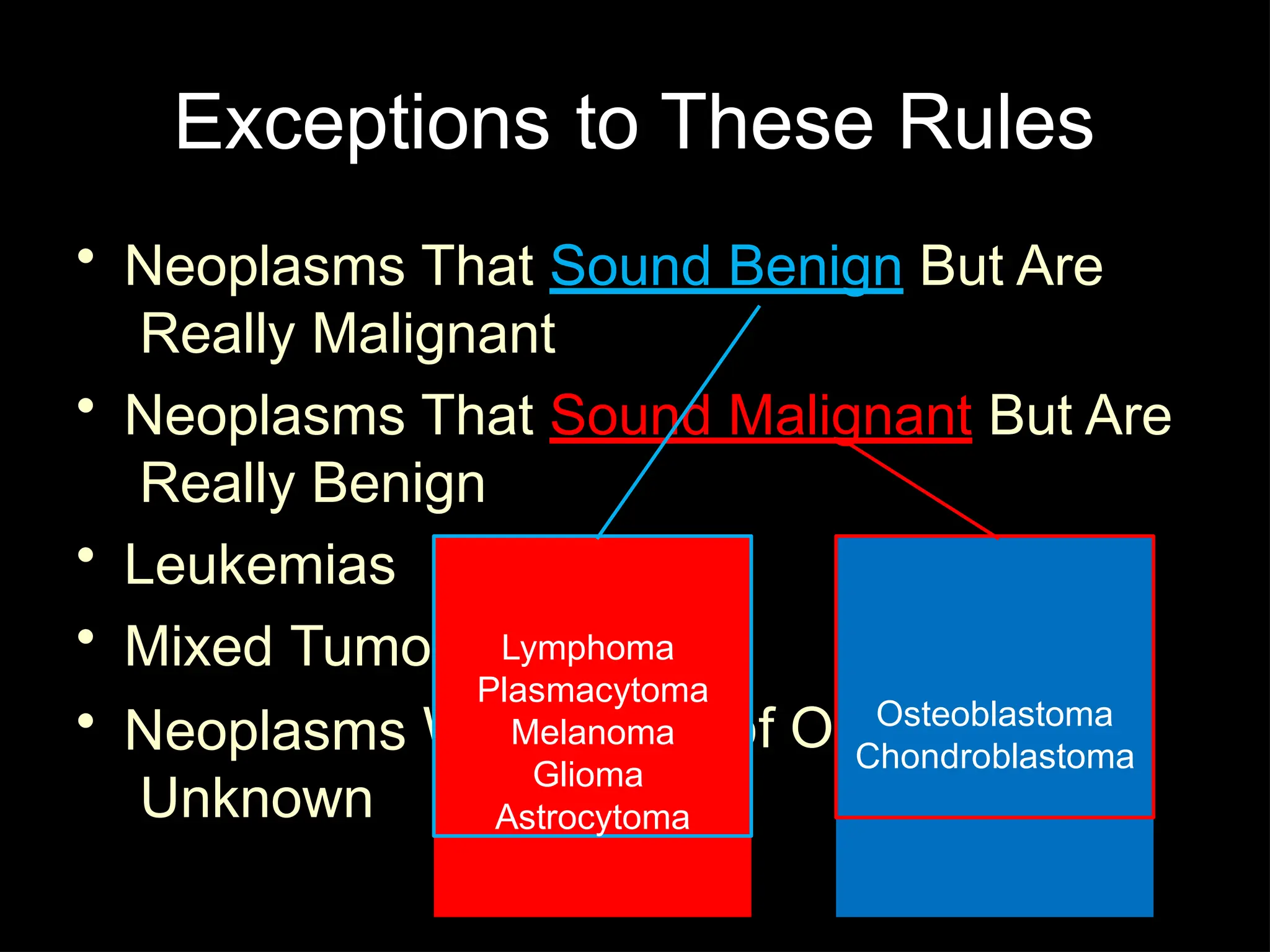
Exceptions to TheseRules
• Neoplasms That Sound Benign But Are
Really Malignant
• Neoplasms That Sound Malignant But Are
Really Benign
• Leukemias
• Mixed Tumors
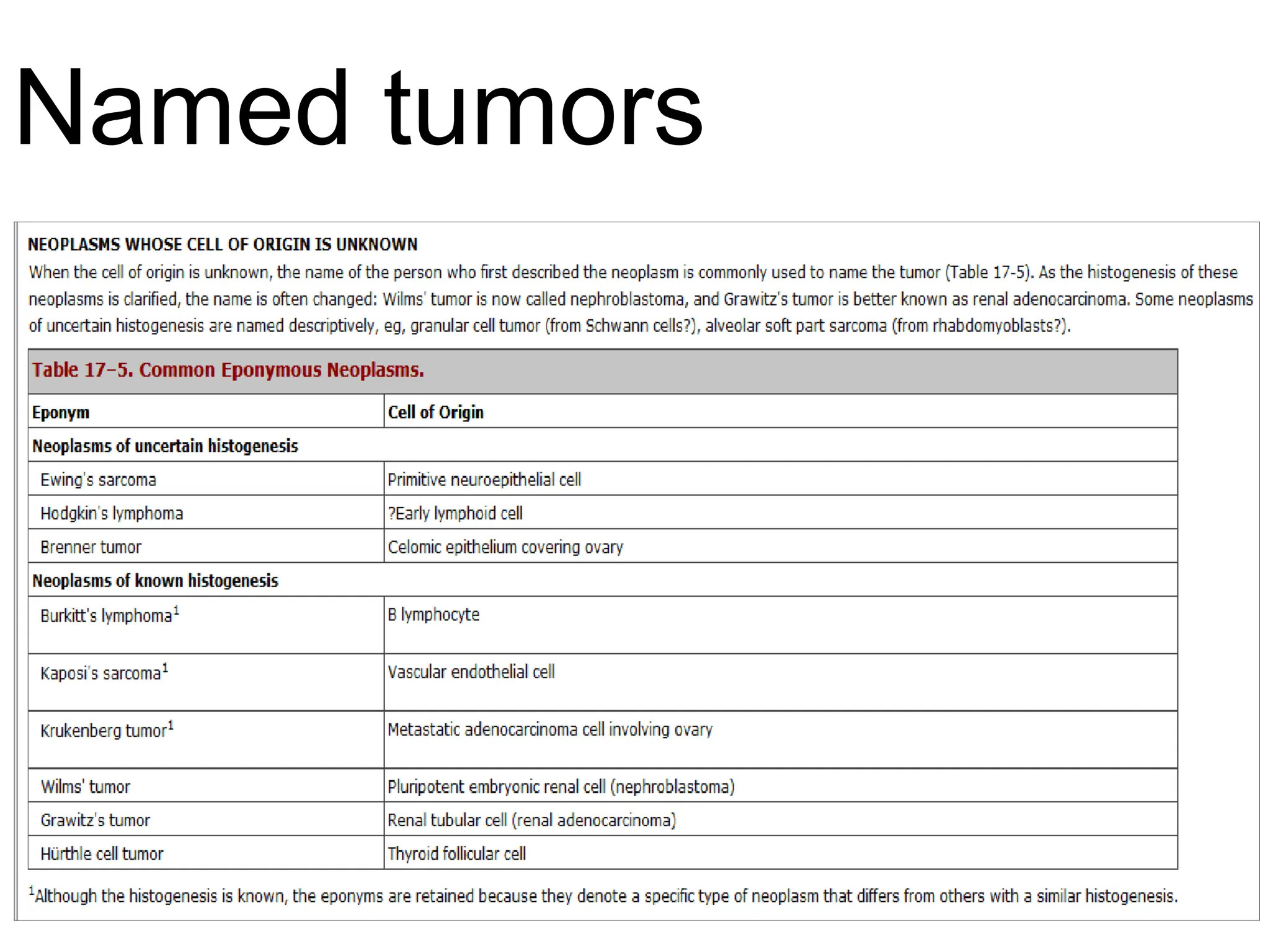
Whose Cell of Origin Is
• Neoplasms
Unknown
Lymphoma
Plasmacytoma
Melanoma
Glioma
Astrocytoma
Osteoblastoma
Chondroblastoma
55.
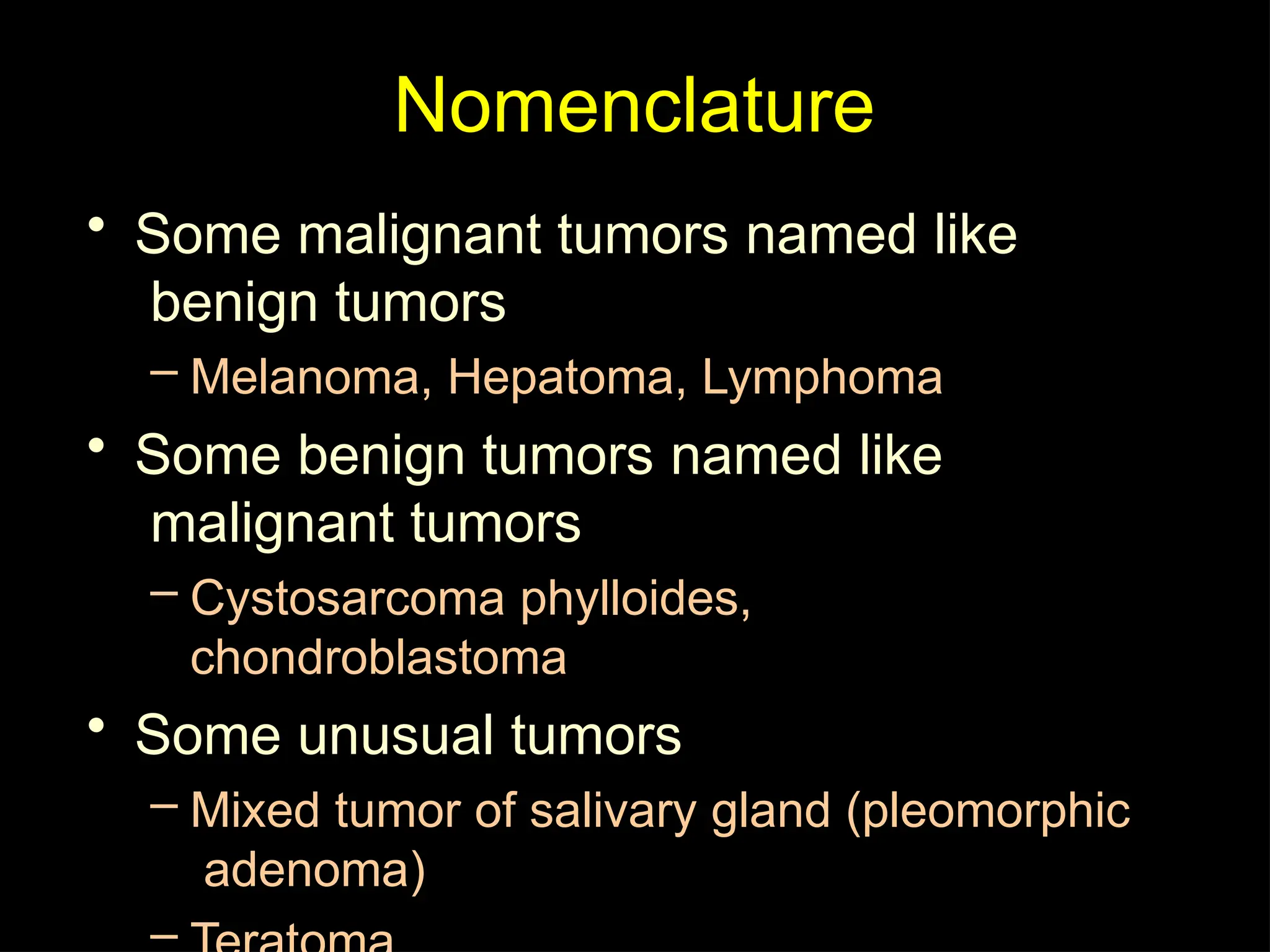
Nomenclature
• Some malignanttumors named like
benign tumors
– Melanoma, Hepatoma, Lymphoma
• Some benign tumors named like
malignant tumors
– Cystosarcoma phylloides,
chondroblastoma
• Some unusual tumors
– Mixed tumor of salivary gland (pleomorphic
adenoma)
–
56.
Mixed tumor
• Tumorswith single type of
parenchymal cells that differentiates
into many cell lines
– Eg: Pleomorphic adenoma of
salivary gland.
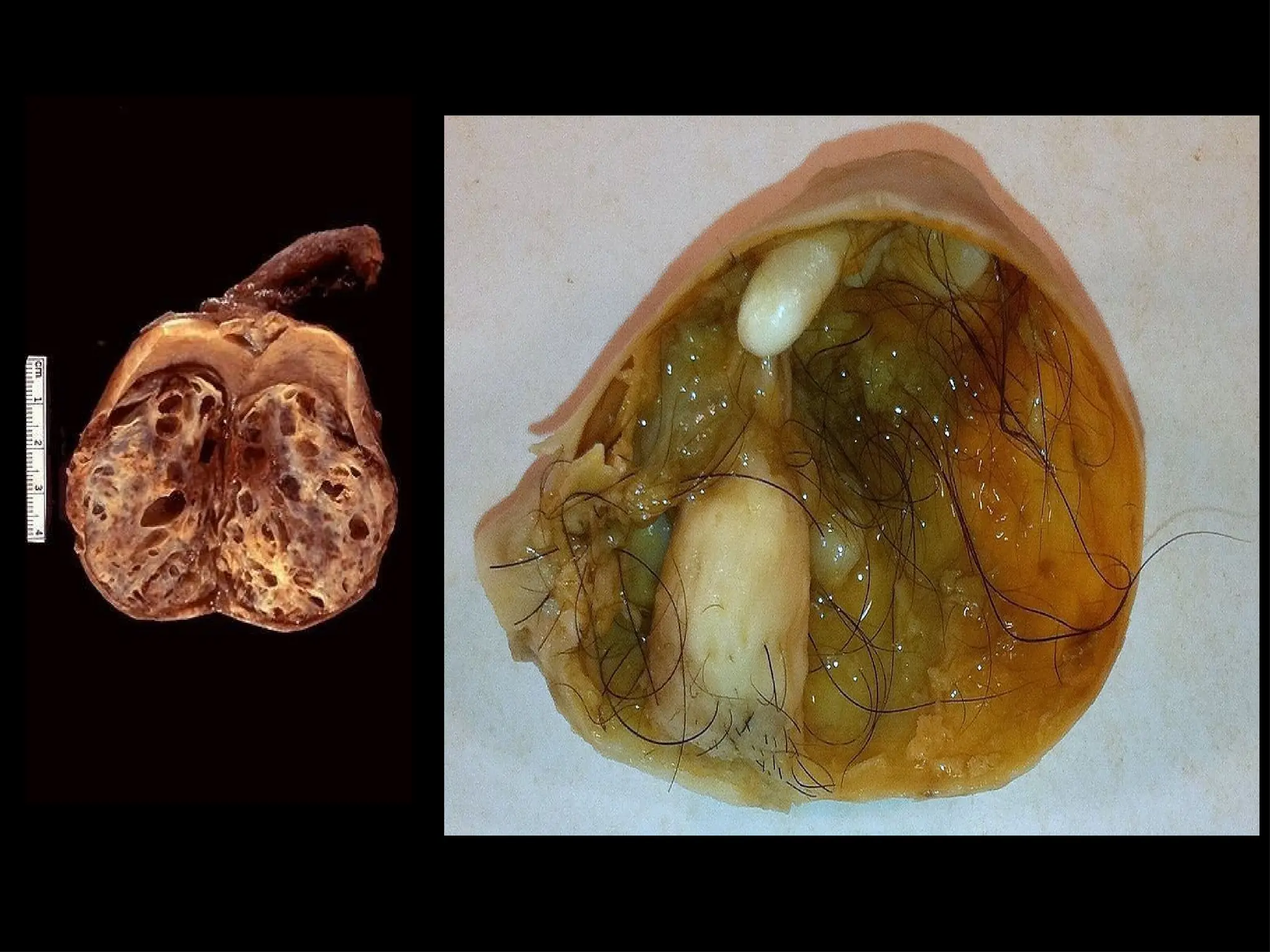
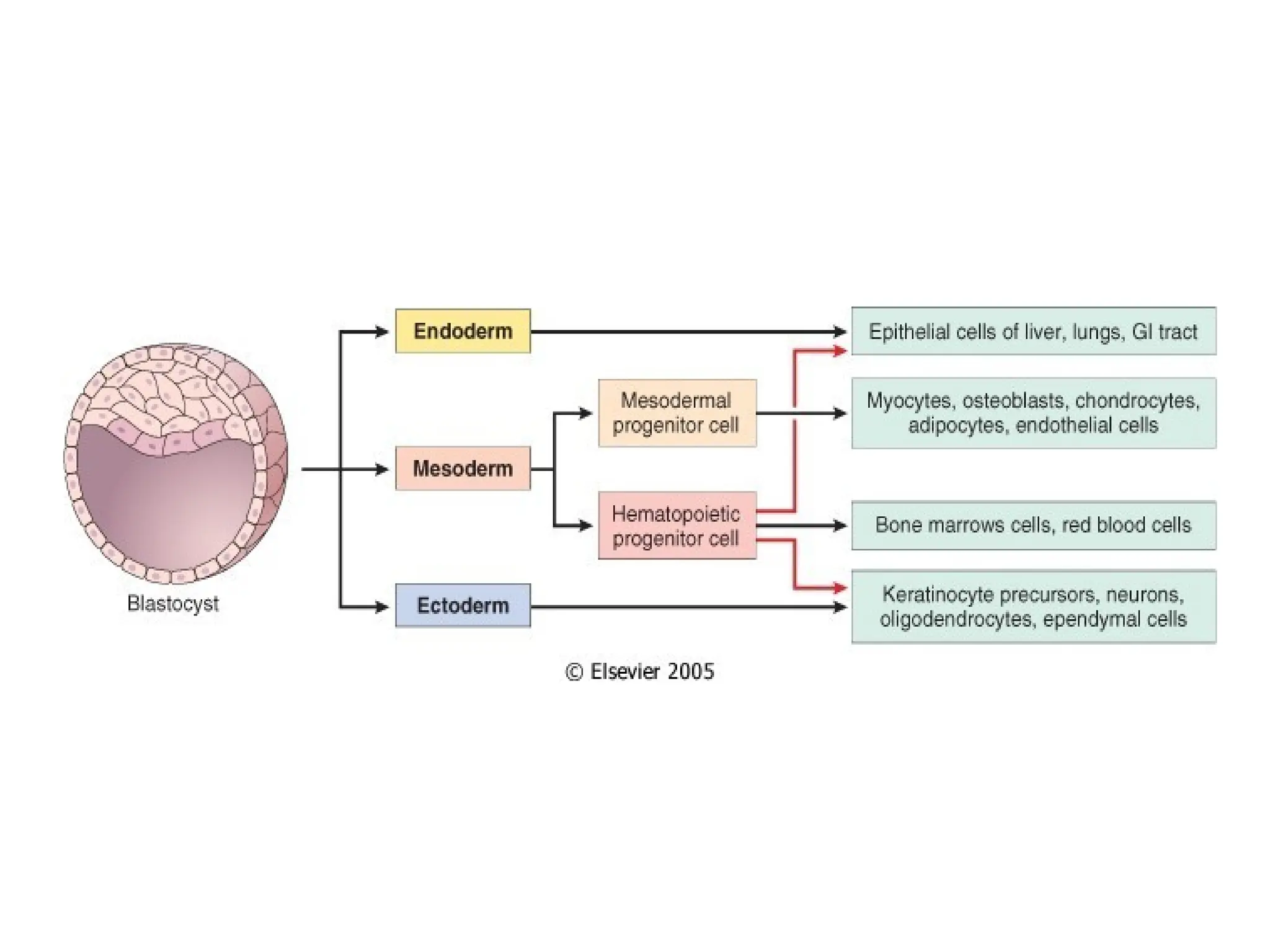
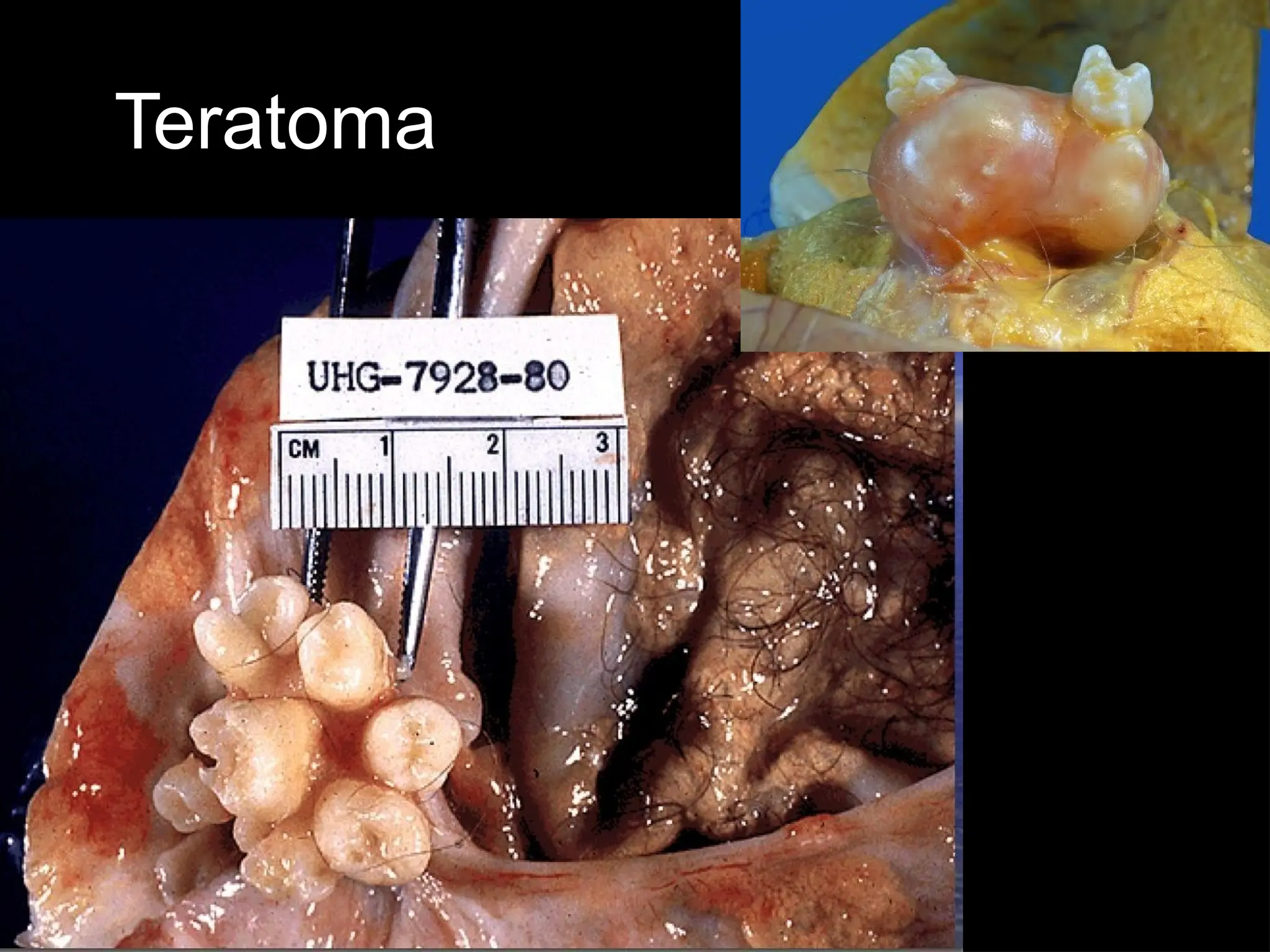
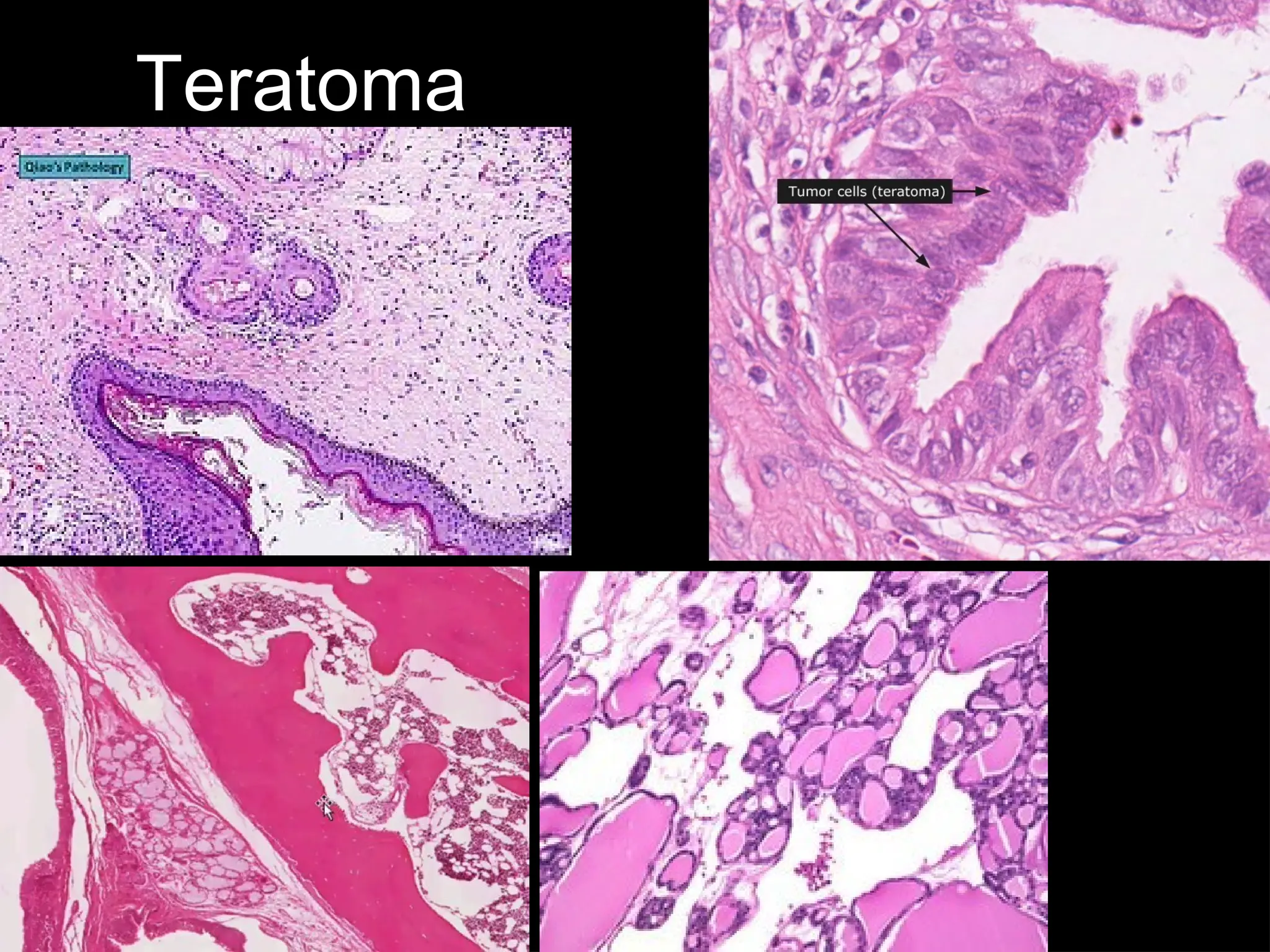
Teratoma
• Tumor arisingfrom totipotent cells (germ
cells) showing differentiation towards
tissues derived from all the three germ cell
layers
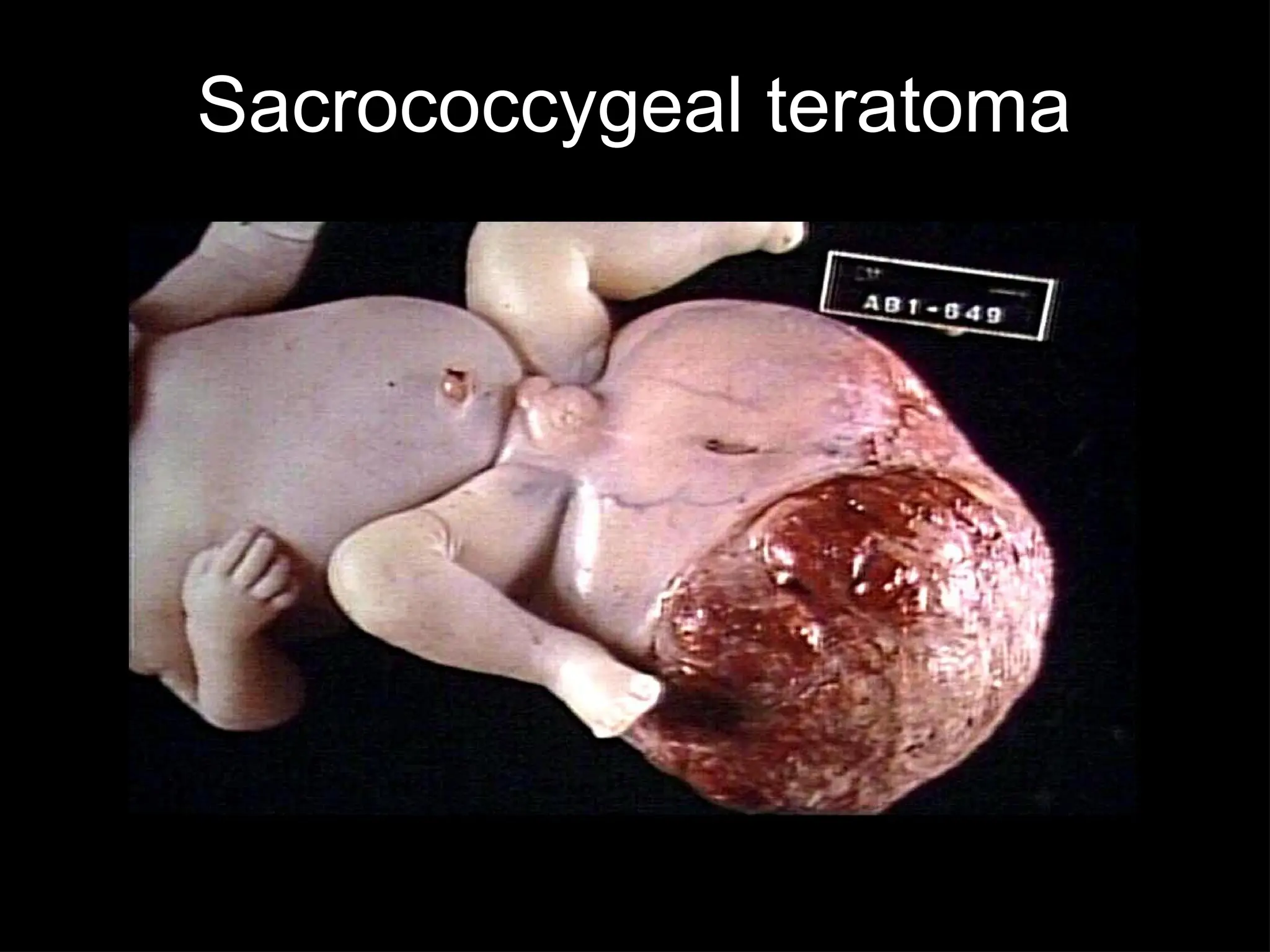
– Seen usually along the midline
– Common sites
• Ovary, testis, sacro-coccygeal region, retro-
peritoneum, mediastinum, base of the brain etc
59.
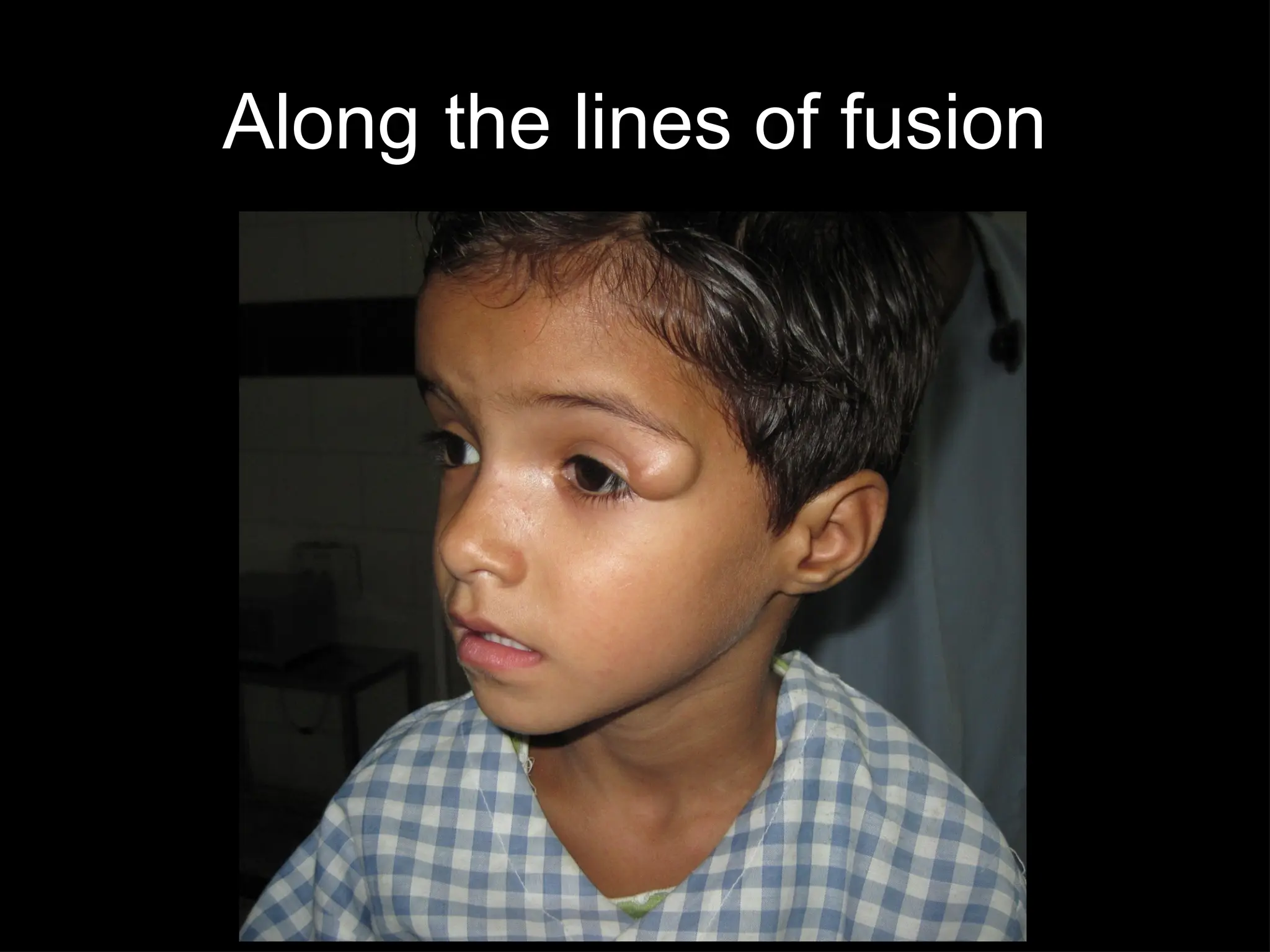
What are thecommon sites for teratomas ?
• Gonads
• Mid line
• Lines of fusion
Hamartomas &
Choristomas
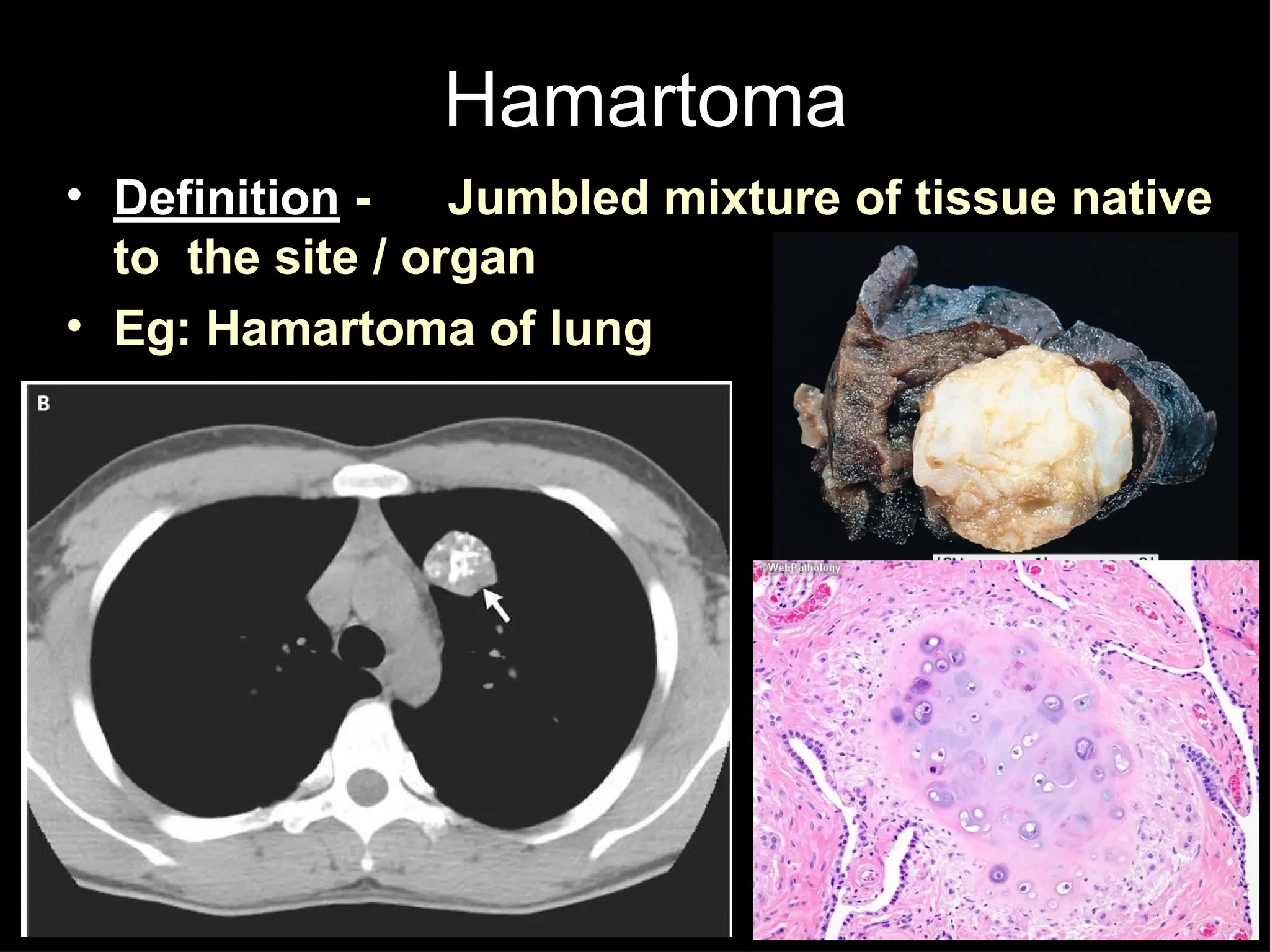
• Ahamartoma is composed of tissues that are
normally present in the organ in which the tumor
arises
– Eg: a hamartoma of the lung consists of a
disorganized mass of bronchial epithelium and
cartilage that may become so large that it presents as
a lung mass. Its growth is coordinated with that of
the lung itself
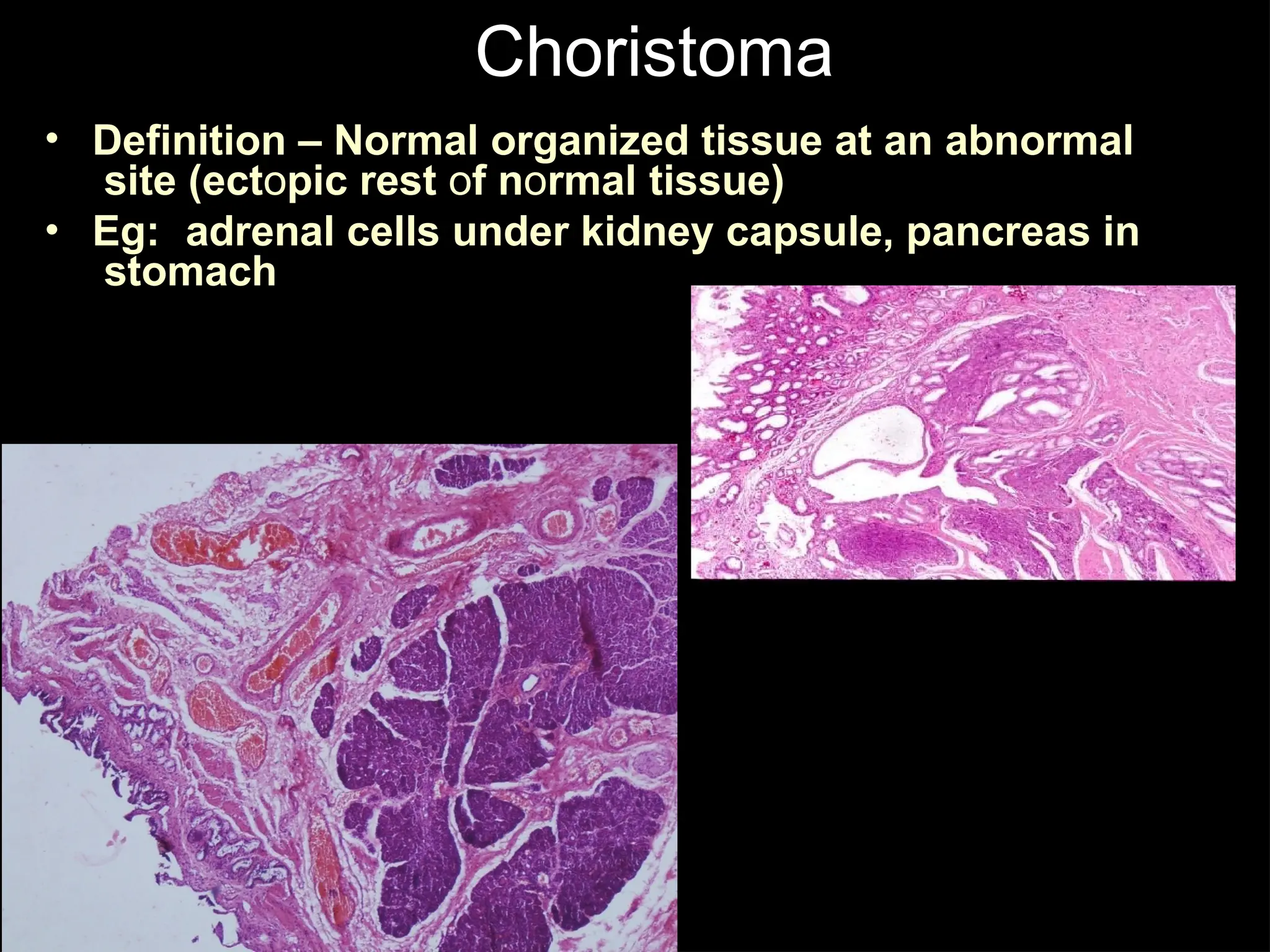
• A choristoma resembles a hamartoma but
contains tissues that are not normally present in
its site of origin
– Eg: A orderly mass of pancreatic acini and ducts in
the wall of the stomach is properly called a
choristoma.
Hamartoma
• Definition -Jumbled mixture of tissue native
to the site / organ
• Eg: Hamartoma of lung
71.
Choristoma
•
•
Definition – Normalorganized tissue at an abnormal
site (ectopic rest of normal tissue)
Eg: adrenal cells under kidney capsule, pancreas in
stomach
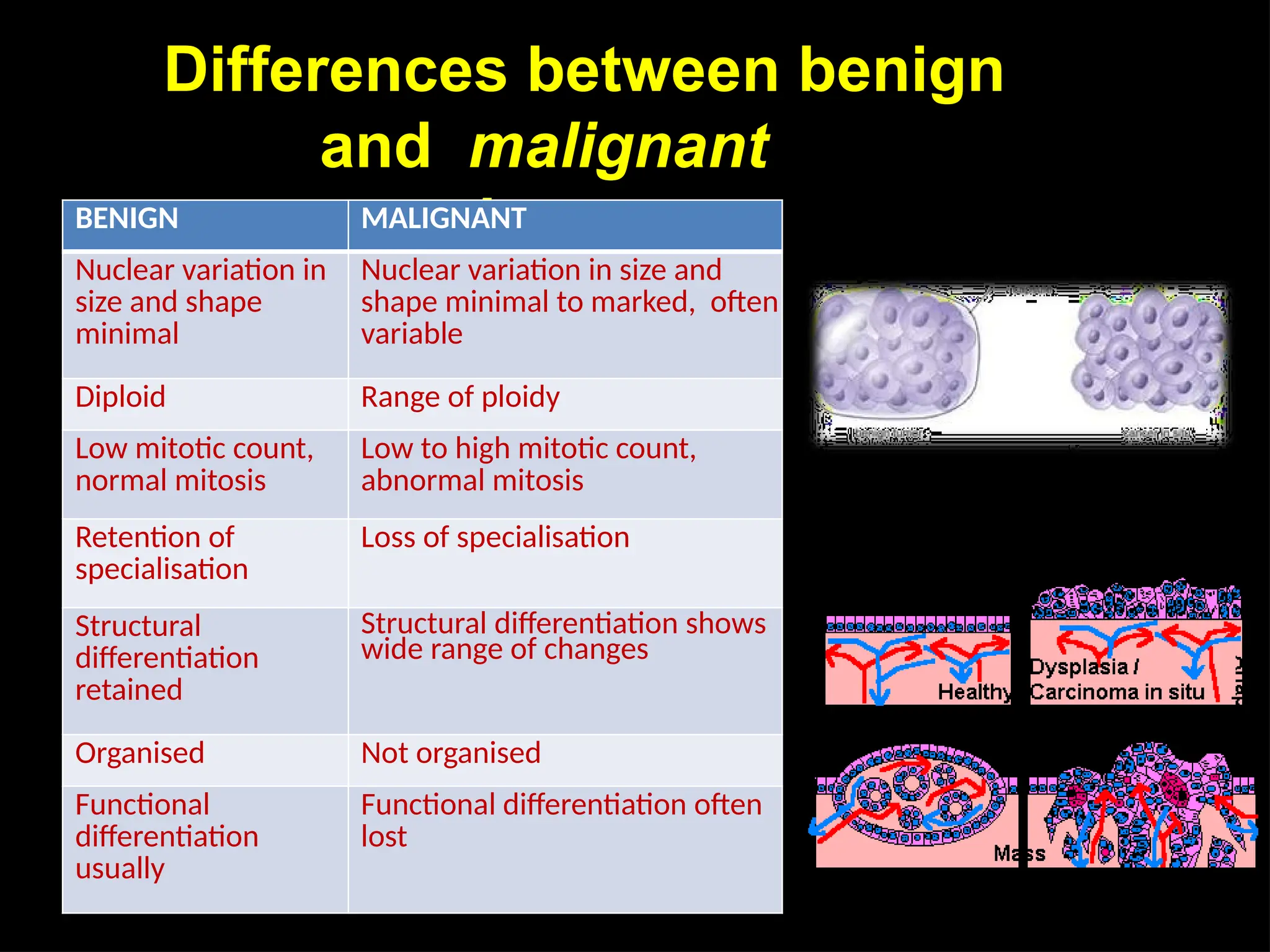
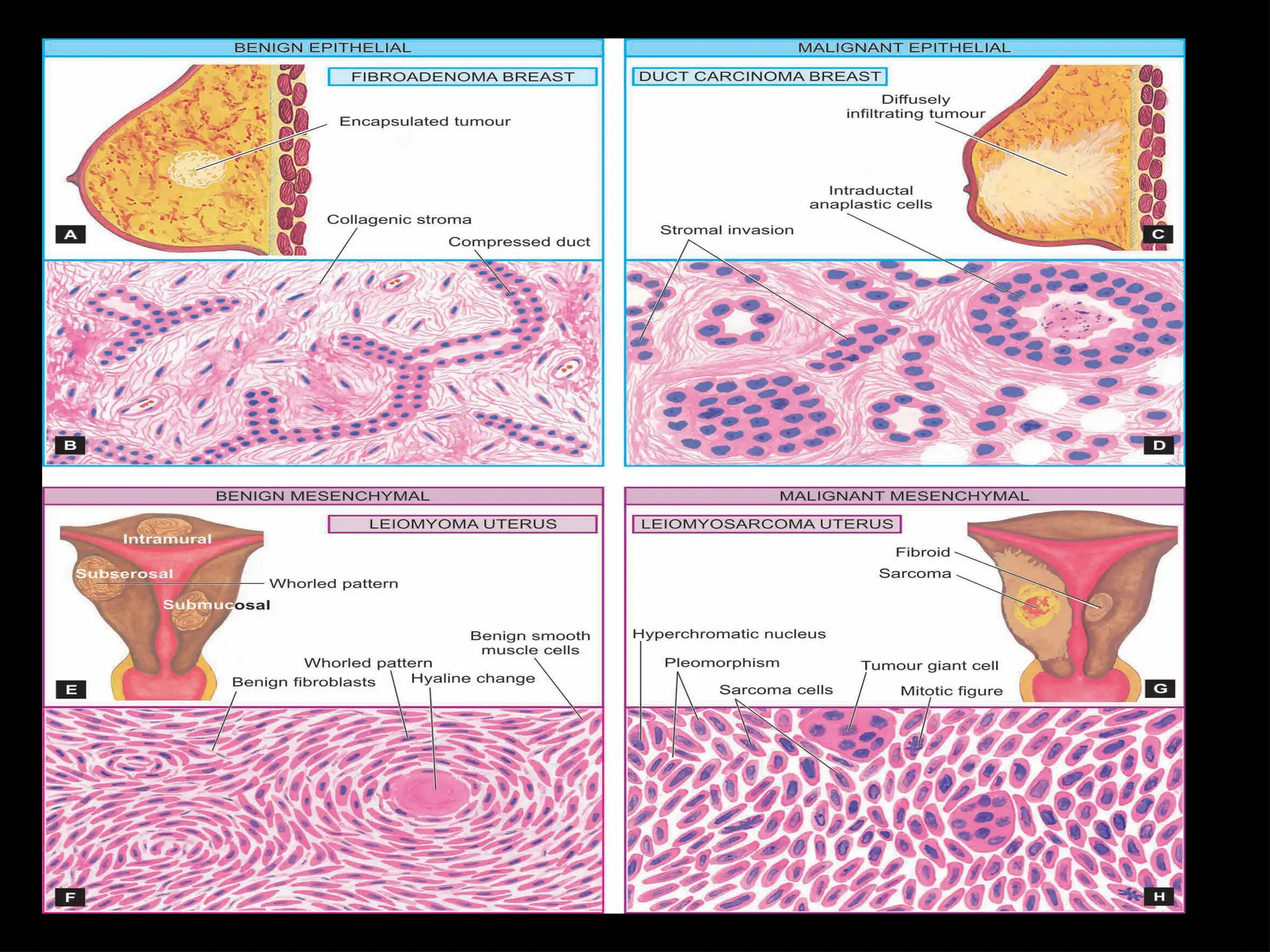
Differences between benign
andmalignant
neoplasms
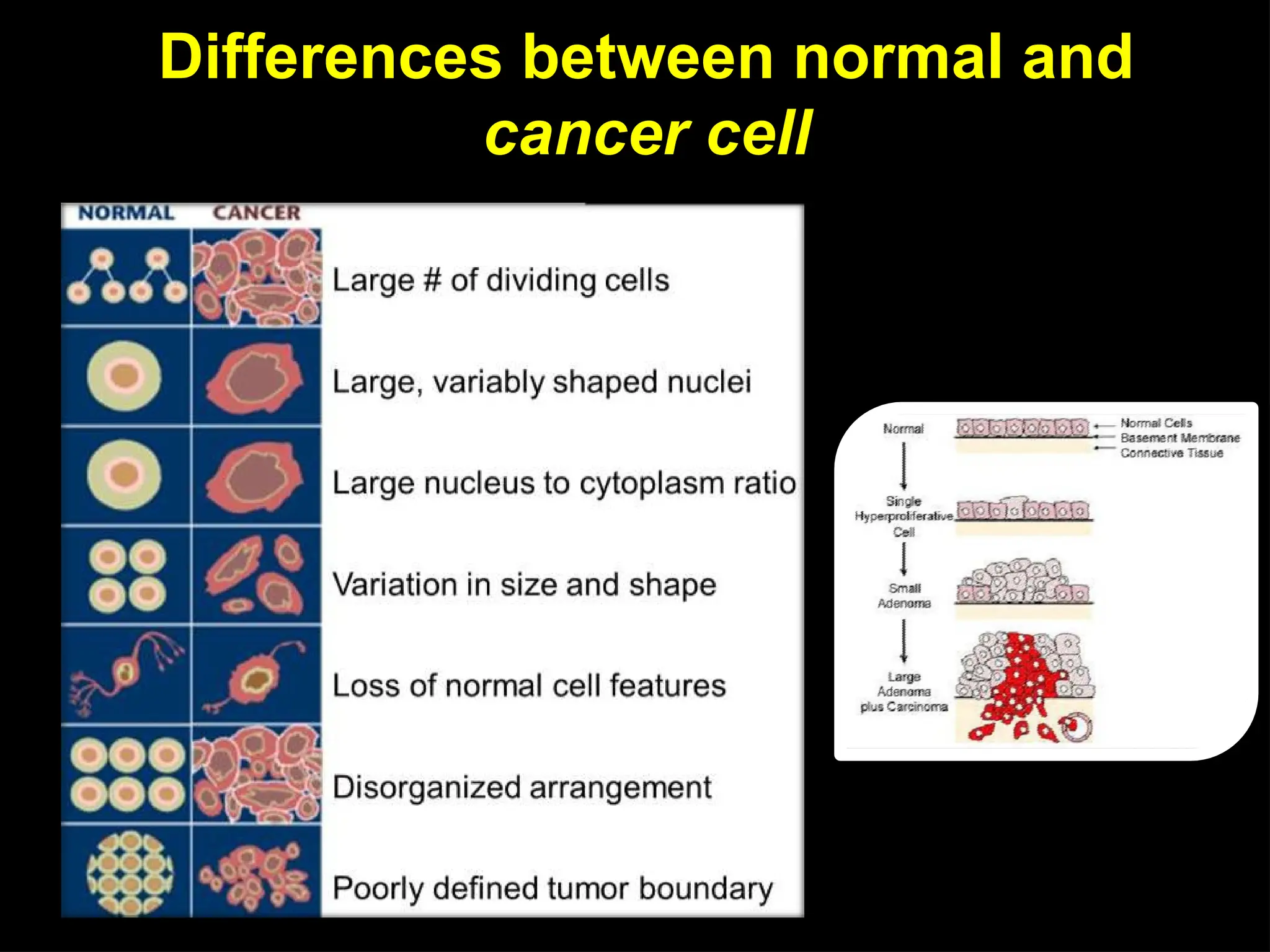
BENIGN MALIGNANT
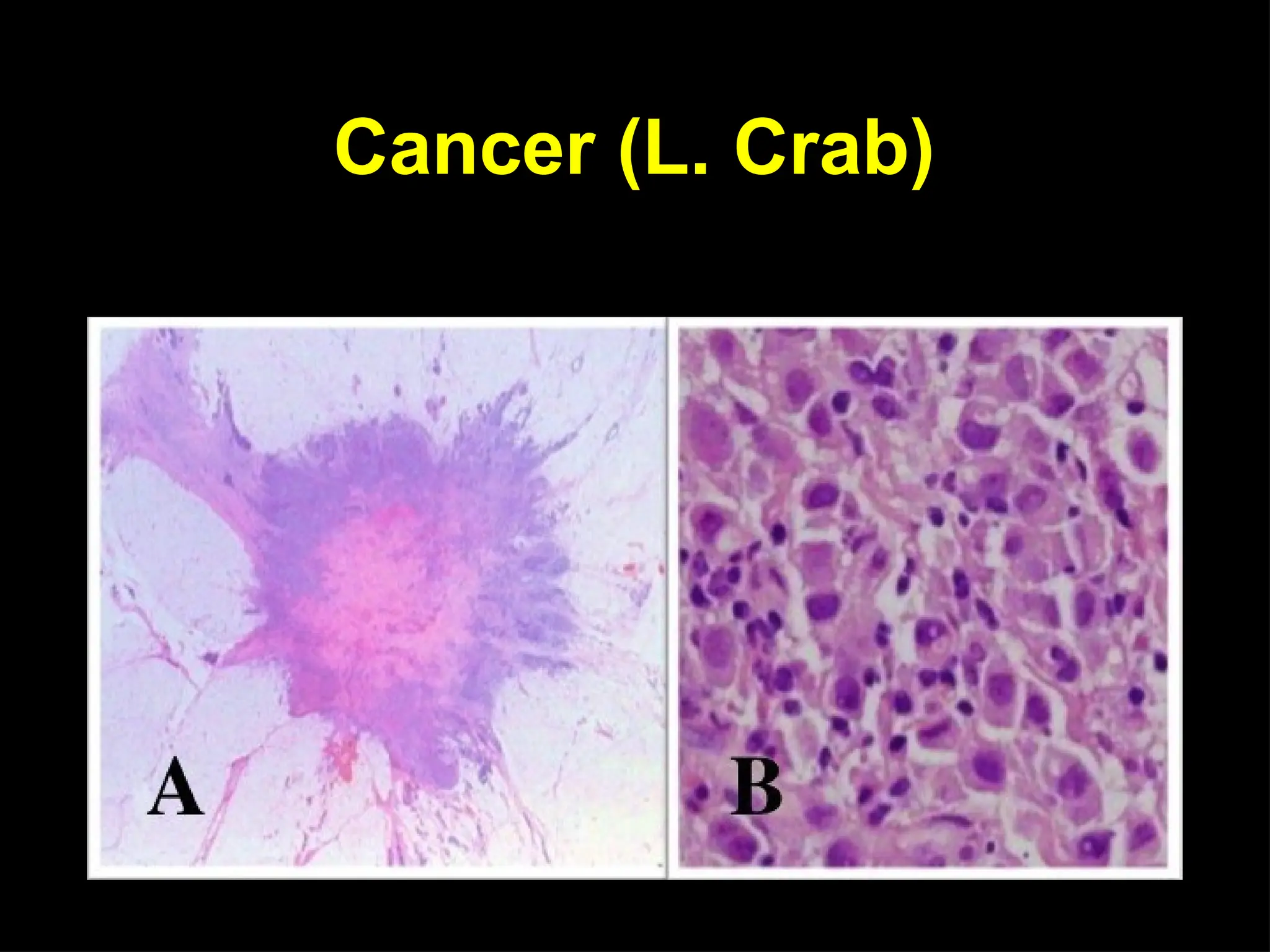
Nuclear variation in
size and shape
minimal
Nuclear variation in size and
shape minimal to marked, often
variable
Diploid Range of ploidy
Low mitotic count,
normal mitosis
Low to high mitotic count,
abnormal mitosis
Retention of
specialisation
Loss of specialisation
Structural
differentiation
retained
Structural differentiation shows
wide range of changes
Organised Not organised
Functional
differentiation
usually
Functional differentiation often
lost
75.
Causes of
cancer
Three majortype of
carcinogens
Chemical carcinogenesis
• Mutagens
• Chemical carcinogenesis and their metabolism
Physical carcinogenesis (radiation)
• Ultraviolet radiation, Asbestos
Infectious Pathogens (Viral)
• Human T-cell leukemia viruses, DNA
viruses, Human papillomaviruses
• Epstein-Barr virus, Hepatitis B virus
76.
Development of cancer
•Changes in DNA (mutation)
• The change must cause an alteration in cell growth and behaviour
• The change must be non-lethal and be passed onto daughter cells
• Alterations in more than one gene
• Genes concerned are oncogenes/tumour suppressor genes
• Sequence of gene alterations from normal to benign to malignant
• Intrinsic and extrinsic / inheritance and environment key factors
77.
Properties of cancercells
• Two unique properties of cancer cells are
– ability to invade locally
– capacity to metastasize to distant sites to distant sites – cancer
spreading (patterns of spread)
78.
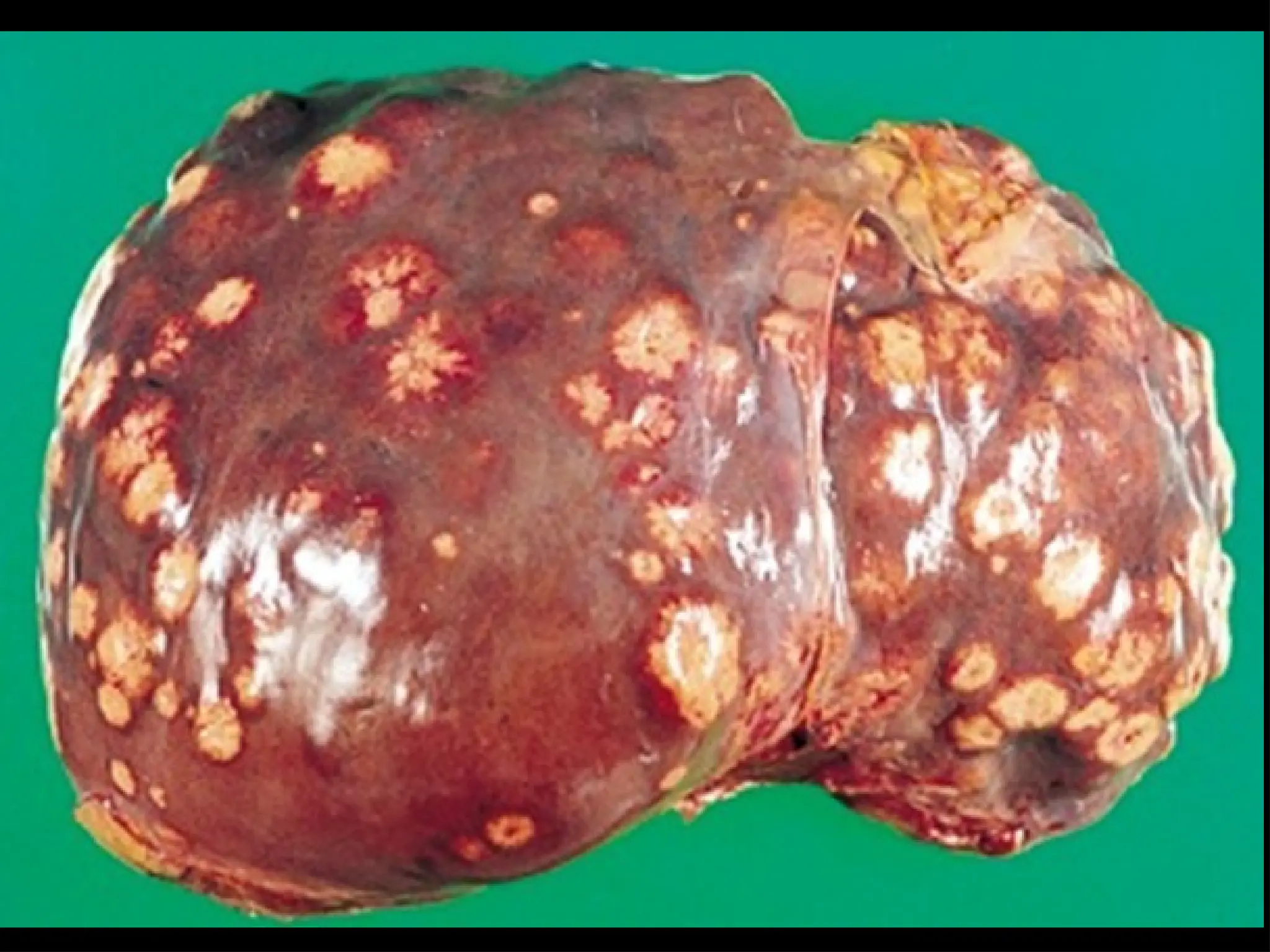
Direct extension: Carcinomasbegin as
localized growths (direct seeding of
body cavities or surface), when they
arise. In early cancers do not
penetrate the basement membrane
(carcinoma in situ). When the in situ
tumor acquires invasive potential
extends directly to compromise
neighboring cells and to metastasize.
E.g. Peritoneal carcinomatosis
(metastatic ovarian carcinoma)
79.
– Metastatic spread:
Transferof malignant cells from
one site to another (not
directly) connected
with it). Invasive properties of
malignant tumors bring them
into contact with blood and
lymphatic vessels.
• Hematogenous metastases
• Lymphatic metastases
80.
Characteristics of tumours
•Majority of neoplasms can be categorized clinically and
morphological into benign and malignant on the basis of
certain characteristics listed bellow
– Rate of growth
– Cancer phenotype and stem cells
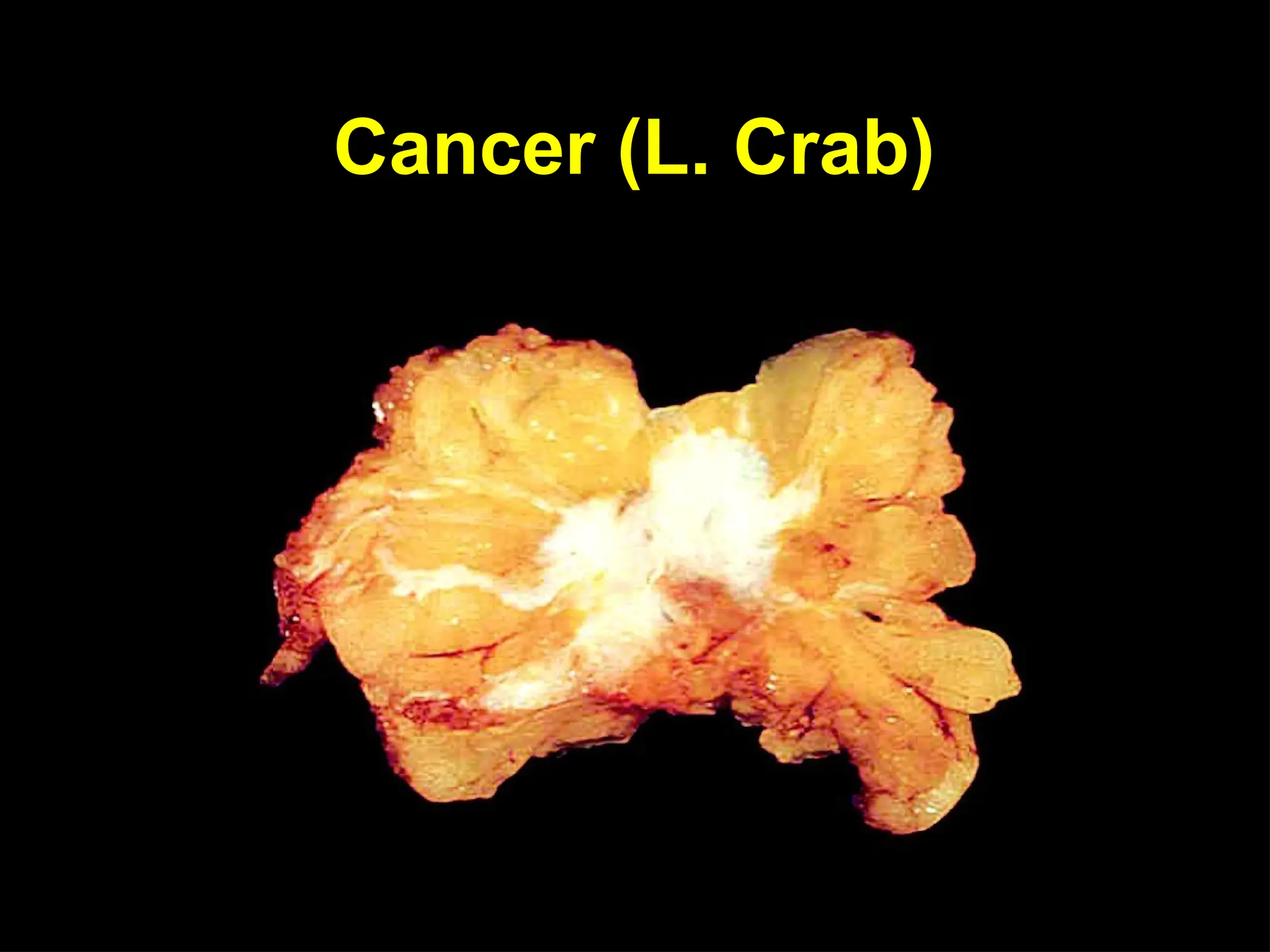
– Clinical and gross features
– Microscopic features
– Local invasion (direct spread)
– Metastasis (distant spread)
81.
• Rate ofgrowth
– The tumour cell proliferate more rapidly
than the normal cells.
– The tumour enlarge rate is depends upon
1. Rate of cell production, growth fraction
and rate of cell loss
2. Degree of differentiation of the tumour
82.
1.Rate of growthof a tumour depends upon
• Doubling time (mitotic rate) of tumour cells
• Number of cells remaining in preoperative pool (growth fraction)
• Rate of loss of tumour cells by cell shedding
Cancer cell do not follow the normal cell controls in cells, and are
immortal. The cell division rate is high and center of tumor do
not receive adequate nourishment and undergo ischemic
necrosis, loss shedding.
Death tumour cells appear as apoptotic figures and dividing
tumours are seen as normal/ abnormal mitotic figure
ultimately tumour grow in size
83.
• Rate ofgrowth
2.Degree of differentiation
• Rate of growth of malignant tumour is directly
proportionate to the degree of differentiation.
• Poorly differentiated tumours show aggressive
growth pattern compare to better
differentiated tumours.
• Rarely, a malignant tumour may disappear
spontaneously from the primary site, due to good host
immune attack.
84.
• Cancer phenotypeand stem cells
Cancer cells
1. disobey the growth control – proliferate rapidly
2. escape from death signals – immortality
3. imbalance between cell proliferation and cell death – excessive growth
4. lose differentiation properties – no function
5. are unstable – newer mutations
6. overrun their neighboring tissue – invade locally
7. have the ability to travel from the site of origin to other part of body
–
distant metastasis
Cancer stem cells/ tumour-initiating cells have the properties of self-renewal,
asymmetric replication and transdifferentiation (i.e. plasticity).
85.
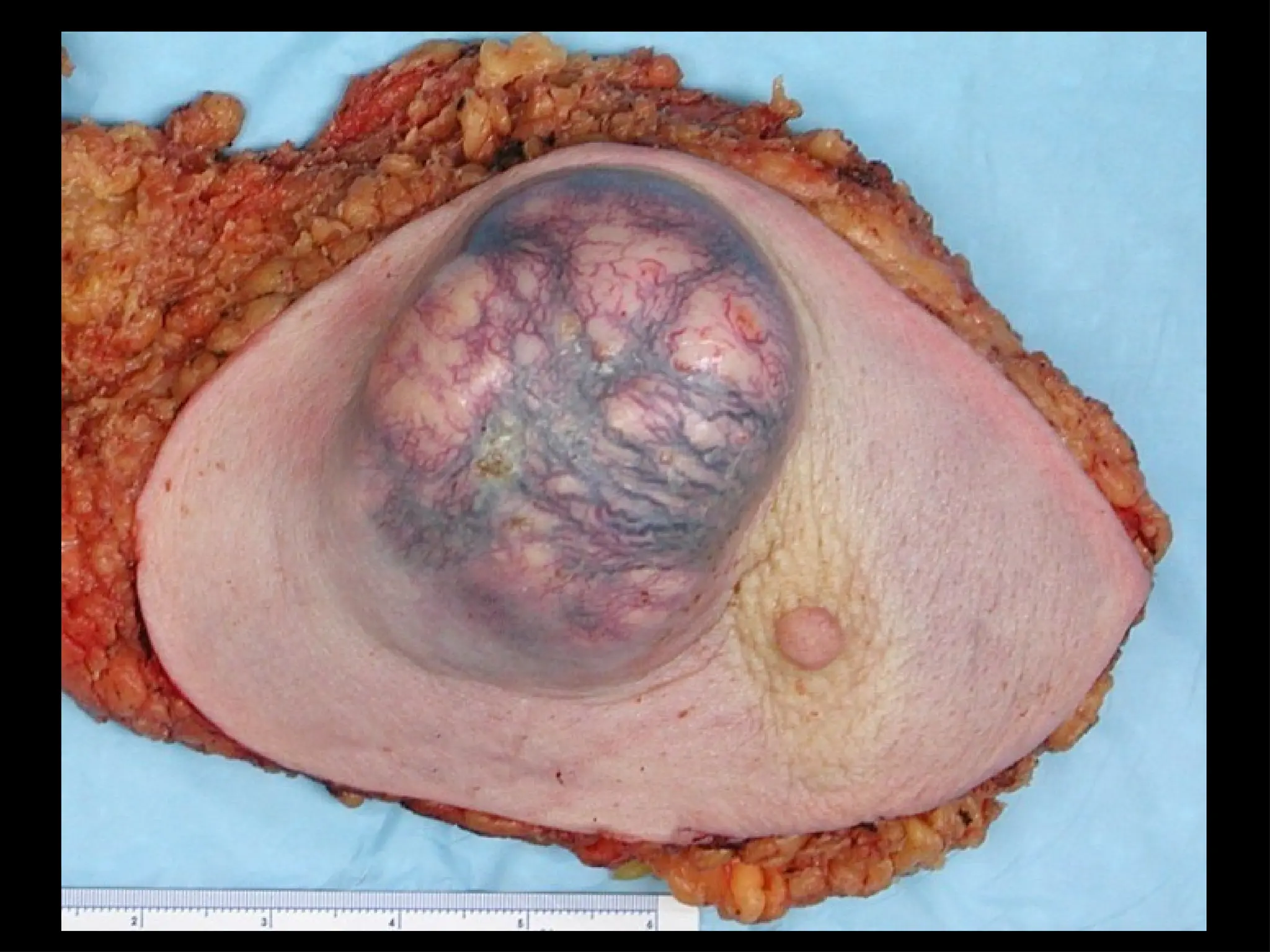
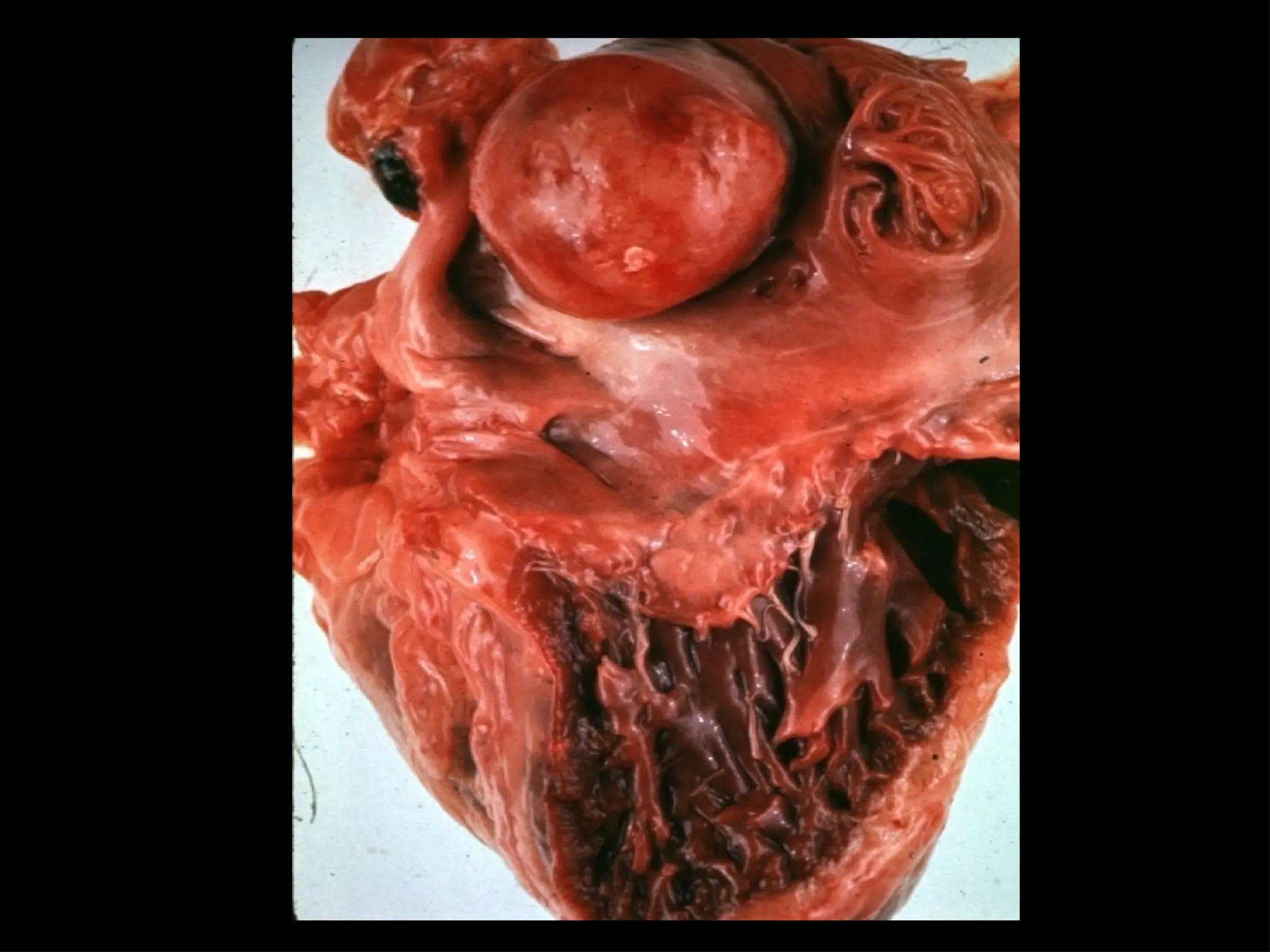
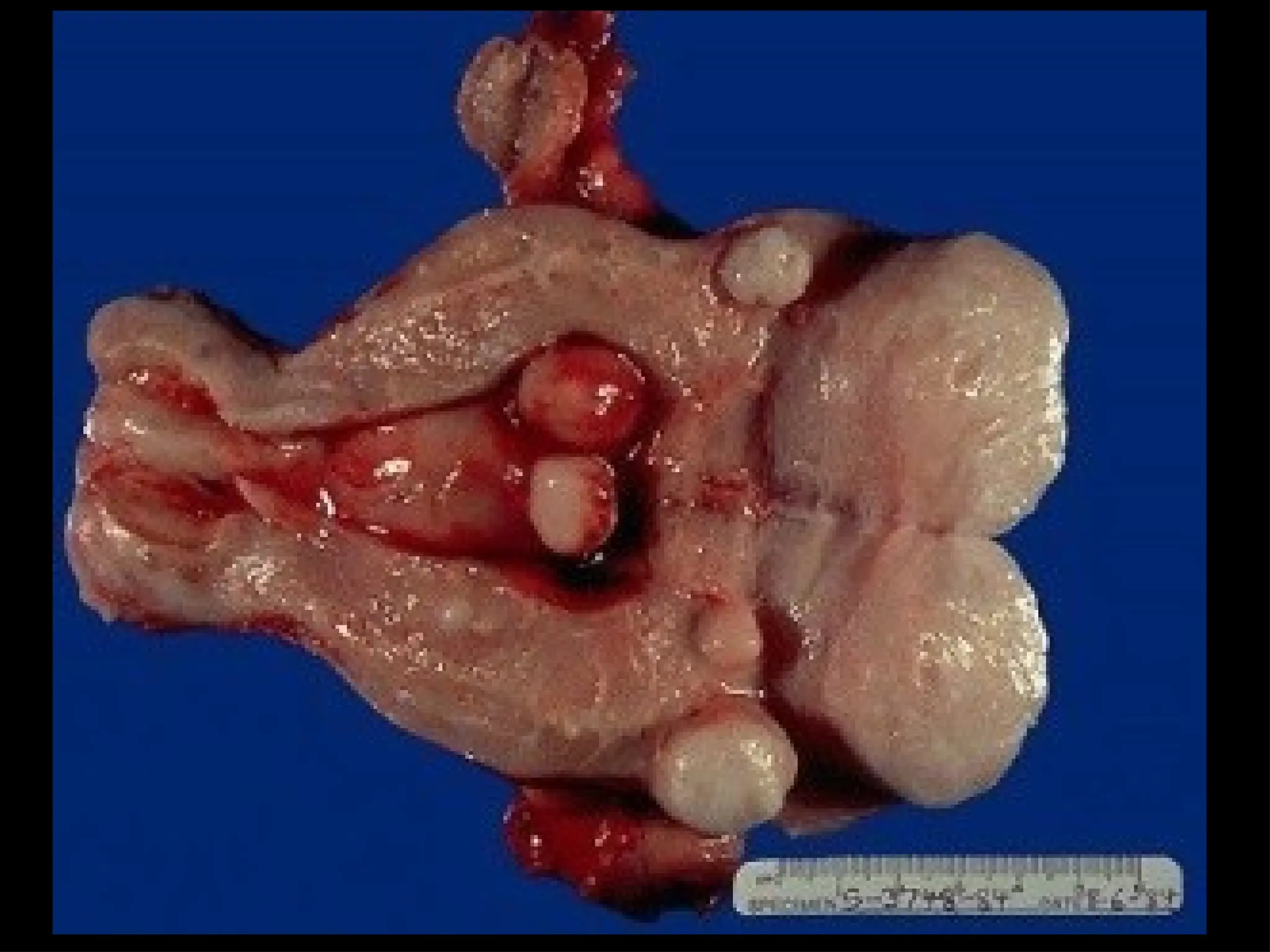
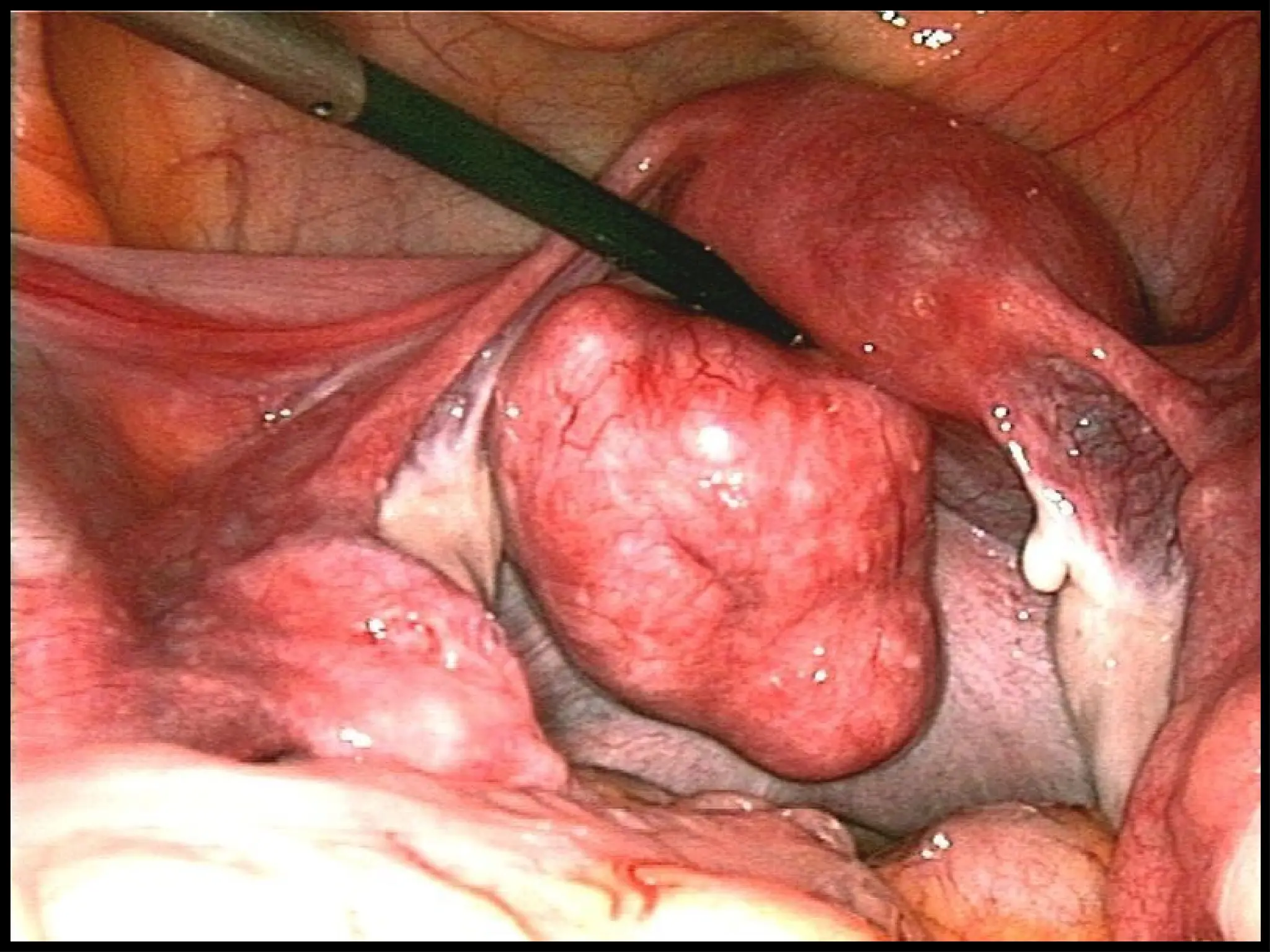
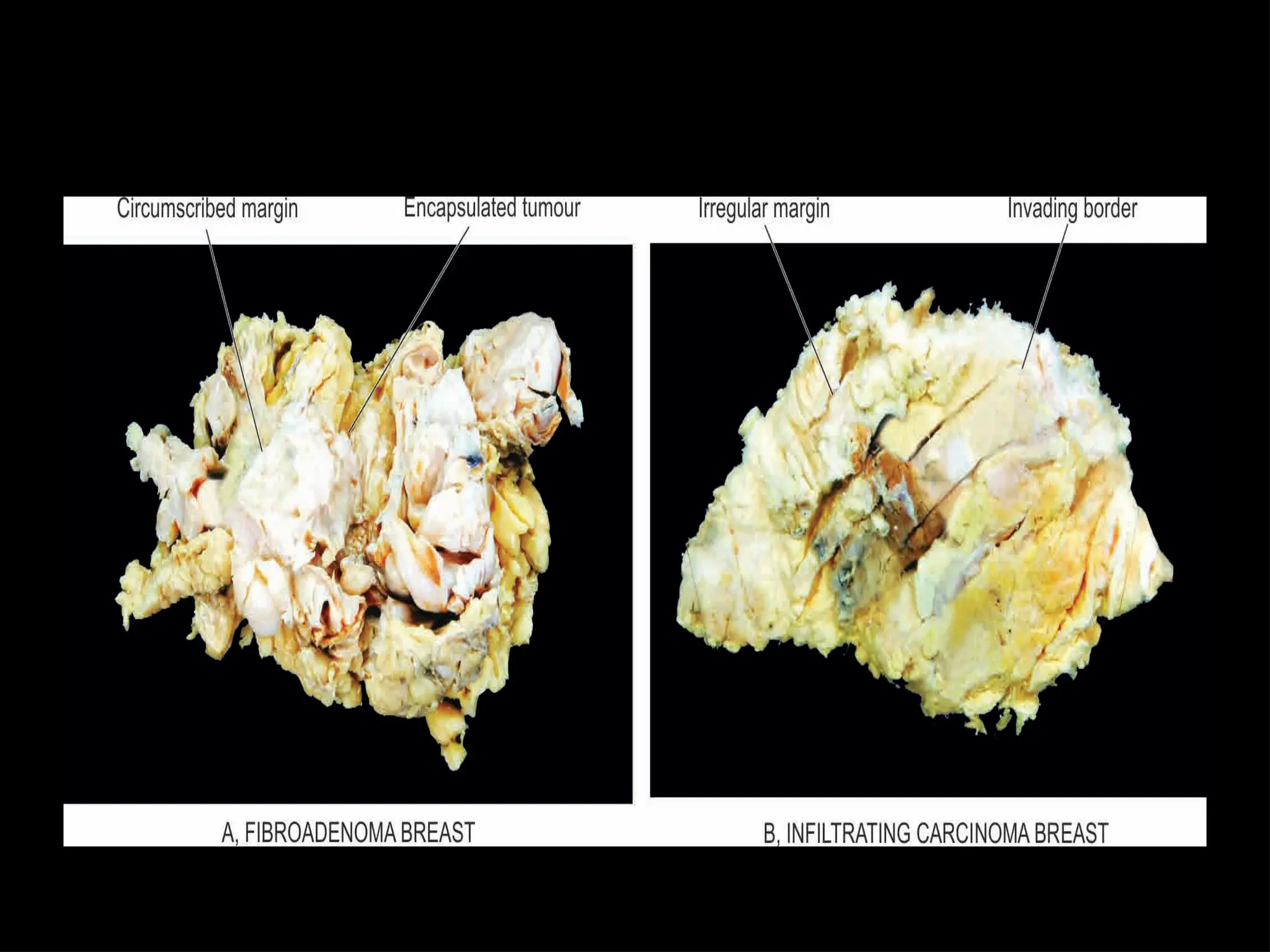
• Clinical andgross features
– Benign tumour are generally slow growing and depending
upon location remains asymptomatic (subcutaneous
lipoma) or may cause serous symptoms (meningioma in the
nervous system). Benign tumours are generally spherical or
ovoid shape.
– Malignant tumor grow rapidly, invade locally into deeper
tissue and spread to distant sites (metastasis). Malignant
tumours are usually irregular in shape, poor-circumscribed
and extend into adjacent tissues.






























![Neoplasia [part 1]](https://cdn.slidesharecdn.com/ss_thumbnails/neoplasiapart1-190918152450-thumbnail.jpg?width=640&height=640&fit=bounds)



























