Downloaded 215 times





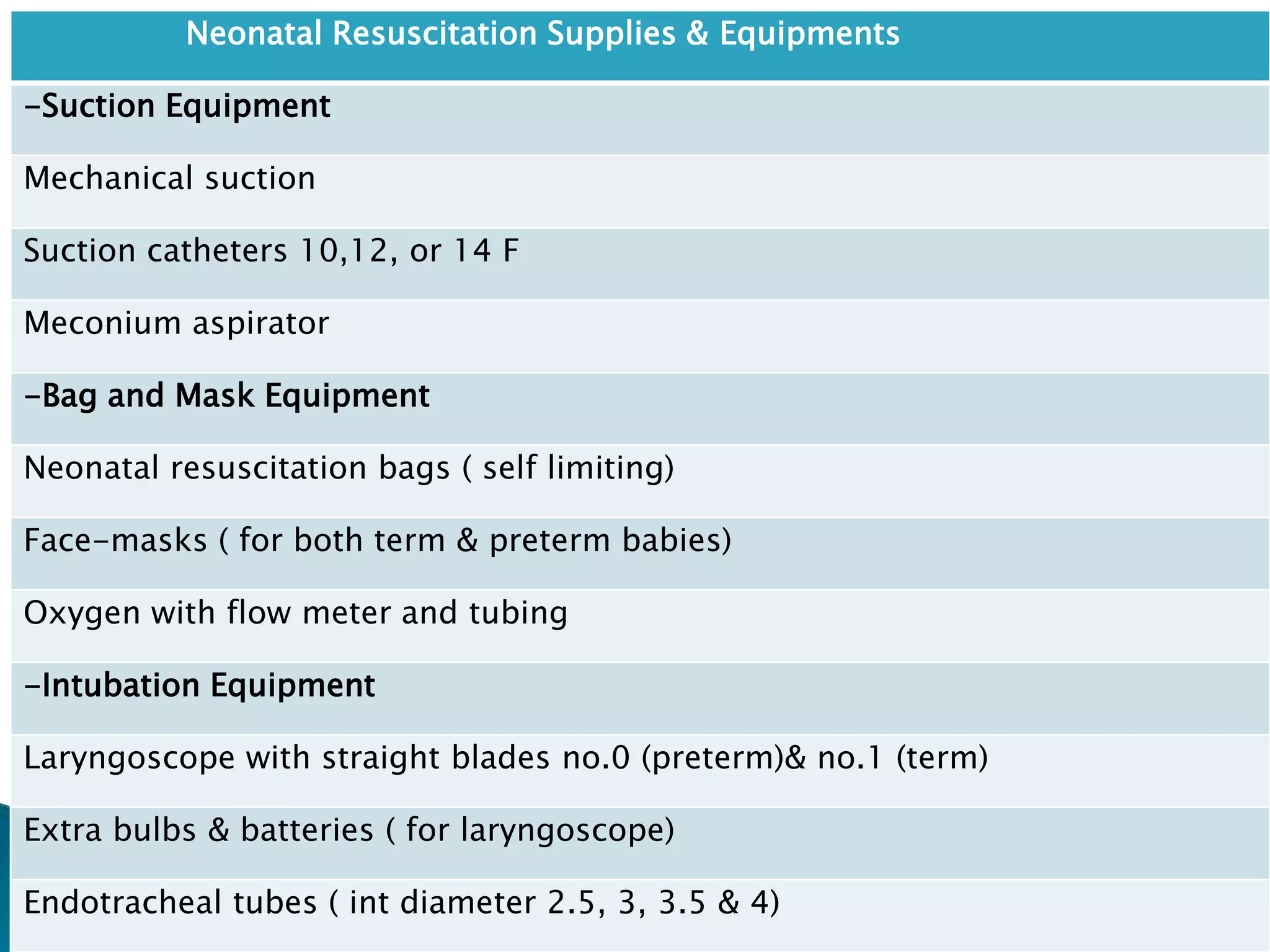













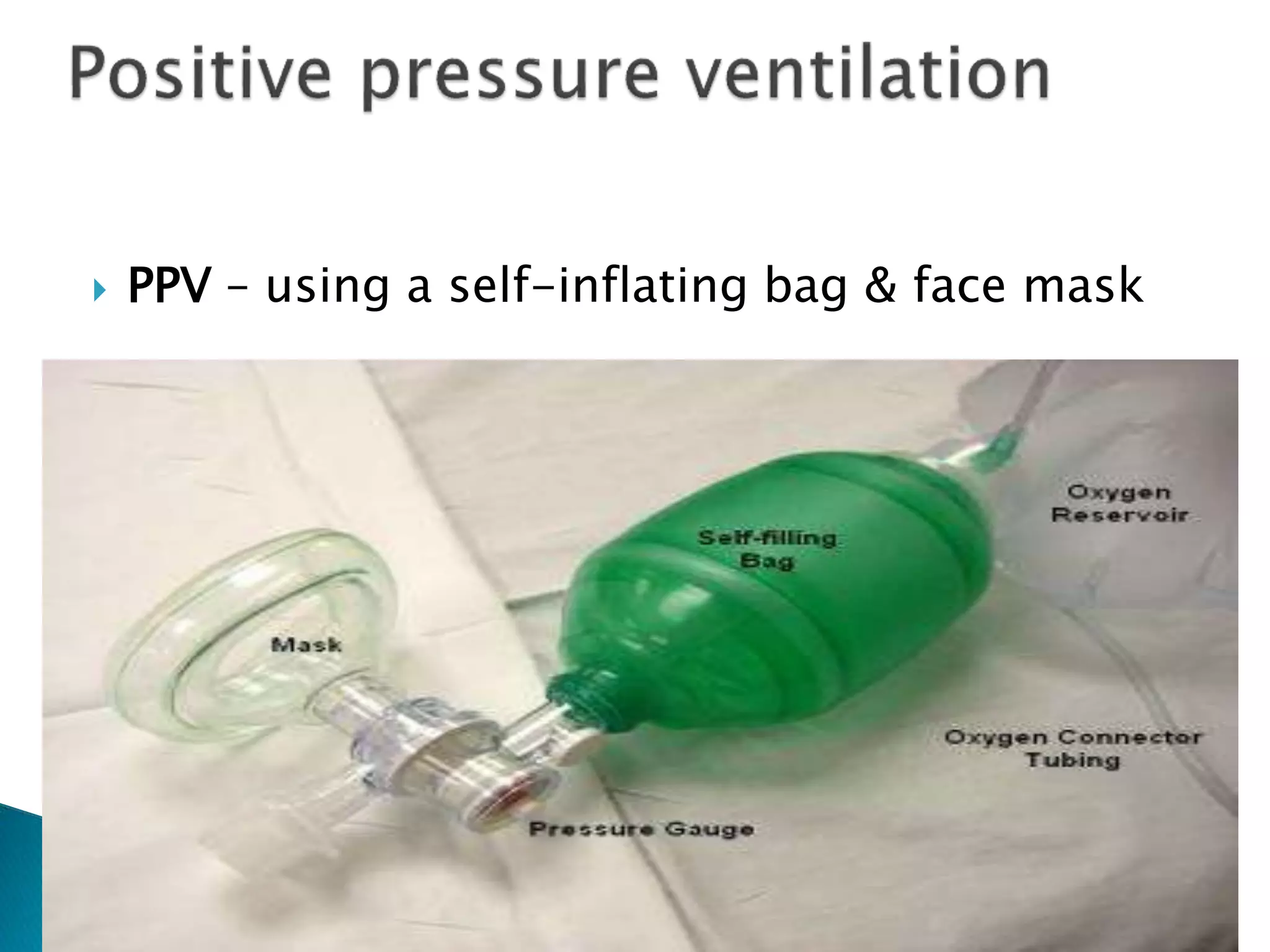






















Neonatal resuscitation is performed to help newborns breathe and for their hearts to beat properly after birth. It is essential for healthcare providers assisting with deliveries. Guidelines from the AHA and AAP are used worldwide in the NRP. Supplies and equipment needed for resuscitation include suction, bag and mask ventilation, intubation equipment, medications, and other miscellaneous items. Assessment of the newborn's breathing, heart rate, tone and color determine if further intervention is needed. Steps may include warming, clearing the airway, stimulation, supplemental oxygen or positive pressure ventilation, chest compressions, and intubation with medications in some cases.



































































