Downloaded 134 times
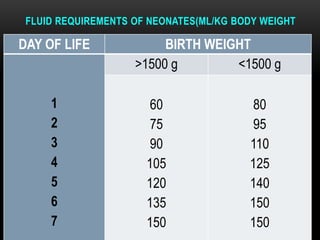
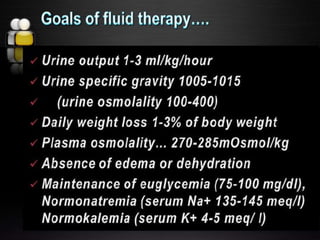
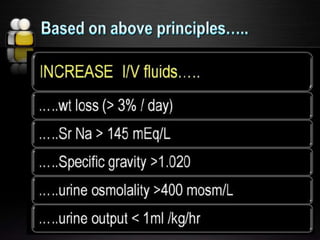


- Neonates requiring IV fluid therapy include those with lethargy/refusal to feed, breathing difficulties, shock, severe asphyxia, or abdominal issues. The aims of fluid therapy are to identify babies needing IV fluids, calculate daily intake, administer measured volumes, and monitor babies receiving IV fluids. Fluid requirements vary based on weight and age, and monitoring includes checking infusion sites, volumes, blood glucose, weight, urine output, and electrolyte levels to properly adjust fluid intake.

































![fluid_and_electrolytes[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fluidandelectrolytes1read-only-250903084601-61978d1f-thumbnail.jpg?width=640&height=640&fit=bounds)

































