DEFINITION
A fractureis a break or
disruption in the continuity of
the bone.
Fractures in children differ from
those in adults
3.
Fracture is commonin
children because of:
Increased mobility
Insatiable curiosity
Immature level of motor co-ordination
Lack of mature judgment about dangerous
situations.
4.
ETIOLOGY
Falls, sports-related injuries,and, less
commonly, child abuse.
Upto age 2, most fractures are sustained as
a result of child abuse. Abuse should be
suspected in this age group
Fractures in newborns are often the result of
child abuse
5.
TYPES OF FRACTURES
Fracturesare divided into three
different categories on the basis of
the following:
Communication with
environment
Pattern
Miscellaneous
6.
Classification on thebasis of
Communication with environment
1. SIMPLE FRACTURE: in this type, skin over the fracture area
remains intact.
2. COMPOUND OR OPEN FRACTURE: the bone is exposed,
through a break in the skin.
3. COMPLETE FRACTURE : in this type, bone is broken across
entirely, destroying the continuity of the bone, resulting in
proximal and distal bone fragments.
4. INCOMPLETE FRACTURE: a fracture that does not entirely
destroy the continuity of bone. This type of fracture is stable
and undisplaced.
7.
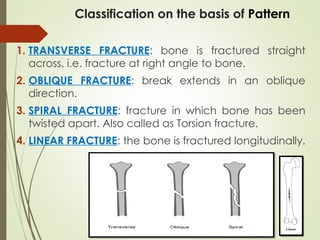
1. TRANSVERSE FRACTURE:bone is fractured straight
across, i.e. fracture at right angle to bone.
2. OBLIQUE FRACTURE: break extends in an oblique
direction.
3. SPIRAL FRACTURE: fracture in which bone has been
twisted apart. Also called as Torsion fracture.
4. LINEAR FRACTURE: the bone is fractured longitudinally.
Classification on the basis of Pattern
8.
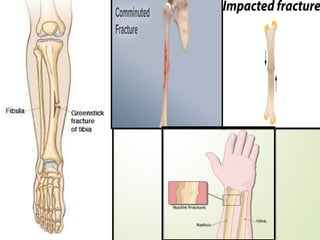
Miscellaneous types
1. GREENSTICKFRACTURE: the bone cracks on one side
but doesn't break all the way through. It is most
commonly seen in children.
2. COMMINUTED FRACTURE: bone is splintered or crushed
with three or more fragments.
3. IMPACTED FRACTURE: a part of fractured bone is driven
into another bone.
4. BUCKLE FRACTURE: one side of the bone buckles or
bends without breaking through entirely.
CLINICAL FEATURES
Pain:Fractures are typically painful, and the pain may
worsen with movement or pressure on the injured area.
Swelling: Swelling around the fracture site is a common
sign, often accompanied by bruising and redness.
Deformity: In some fractures, particularly those involving
long bones, a visible deformity or an unusual angle of
the limb may be apparent.
Limited Mobility: Children may be unable or reluctant to
move the injured limb or put weight on it.
12.
Bruising: Bruisingaround the fracture site is common due to
blood vessel damage.
Open Fractures: In some cases, the broken bone may protrude
through the skin, creating an open wound.
Inability to Move the Limb: A child may not be able to move
the affected limb or may refuse to use it.
Warmth, Redness, or Bruising: These signs may also be present in
the affected area.
Inability to Put Weight on the Affected Area: A child may be
unable to bear weight on the affected limb or avoid doing so.
CLINICAL FEATURES
13.
DIAGNOSTIC EVALUATION
Complete history
Clinicalmanifestations
X-ray
CT scan
Lab diagnosis :
Hemorrhage due to severe injury leads to
decreased Hb.
Elevation in WBC count due to inflammation.
14.
MANAGEMENT OF
FRACTURES
Major Objectives:
Torestore fracture fragments to their normal
anatomic position (reduction)
To maintain bone fragments in place until
healing occurs (immobilization)
To help children regain normal functions and
strength of the affected part (rehabilitation)
15.
MANAGEMENT
1.FRACTURE REDUCTION:
Fractures arereduced, before edema occurs and
tissues are infiltrated by hemorrhage.
Method used for fracture reduction depends on:
Child’s age
Status of bone
Condition of skin and soft tissues
Status of neurovascular functioning
16.
FRACTURE REDUCTION METHODS
CLOSED REDUCTION: It is accomplished by bringing bone fragments
into apposition (ends in contact) by manipulation and traction.
TRACTION: traction is pulling force applied in a longitudinal direction
to reduce a fracture. It can also be used to immobilize a fracture.
OPEN REDUCTION: some fractures require surgery or open reduction
so that the bone fragments can be repositioned under direct
visualization.
Internal fixation devices like metallic screws, plates or rods may be
used to hold fragments of bone in position until solid bone healing
occurs.
18.
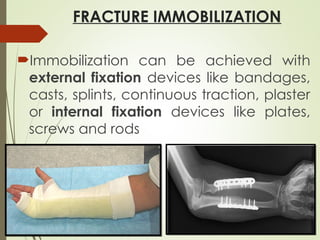
FRACTURE IMMOBILIZATION
Immobilization canbe achieved with
external fixation devices like bandages,
casts, splints, continuous traction, plaster
or internal fixation devices like plates,
screws and rods
19.
NURSING MANAGEMENT
Nursing managementof children while application of casts:
1.Before the cast is applied, extremities are checked for presence of rings
or other items that might cause constriction from swelling, so these are
removed.
2.Care should be taken to forma smooth-padded edge to protect skin
rom injury by hard cast edges.
3.Cast must be kept uncovered until it dries from inside out.
4.A fan can be used to circulate air around the cast.
5.A dryer or heated fan should not be used because the outside of the
cast would dry before inside, resulting in burns due to heat conduction
from cast to skin.
20.
Nursing management ofchildren while application of casts:
Prevention of circulatory, neurologic or respiratory disturbances.
Wet cast is supported with palms of hands and not finger tips, to
prevent denting the cast that may cause pressure on underlying
skin.
The casted lower extremity is elevated and supported on plastic
covered pillow, avoiding pressure on the heel.
The casted upper extremity is elevated and supported on plastic
covered pillow or in sling suspension around the child’s neck.
21.
Nursing management ofchildren
while application of casts
Maintenance of body temperature
Maintenance of skin integrity and prevention
of infection
Maintenance of cleanliness
Promotion of appropriate muscle activity
Provision of comfort measures
Prevention of urinary statis and constipation
Education of parents and child.