The document summarizes several national health programs launched by the Government of India:
1) The National Mental Health Programme aims to prevent and treat mental disorders and improve access to mental healthcare. It integrates services into primary care.
2) The National Guinea Worm Eradication Programme aims to eliminate guinea worm disease through surveillance, case management, water treatment, and health education. India was certified guinea worm free in 2001.
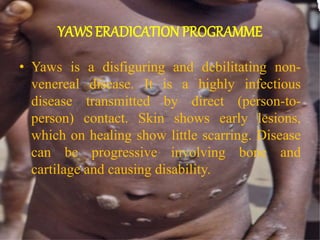
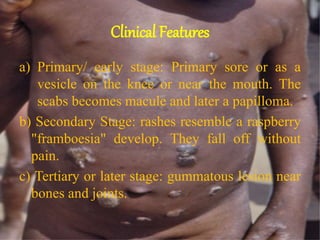
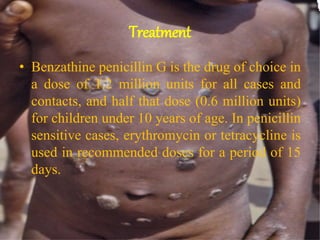
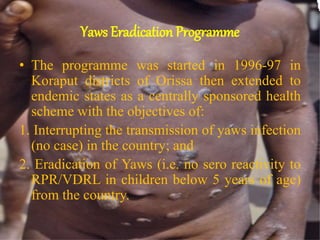
3) The Yaws Eradication Programme aims to end transmission and eliminate yaws through treatment of cases and contacts with penicillin.
4) The National Programme for Control and Treatment of Occupational Diseases funds research on common workplace hazards like silicosis.