Downloaded 103 times
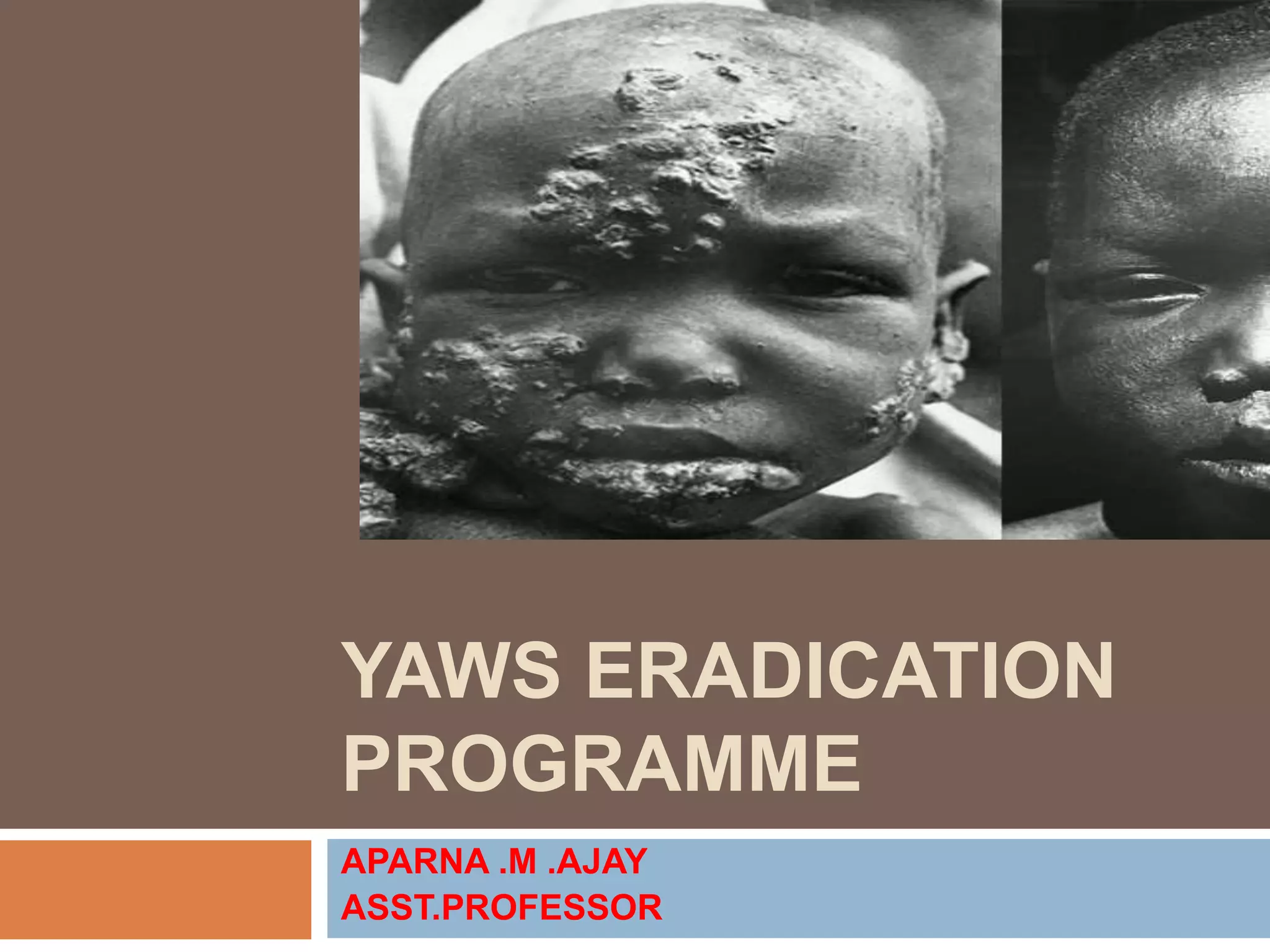












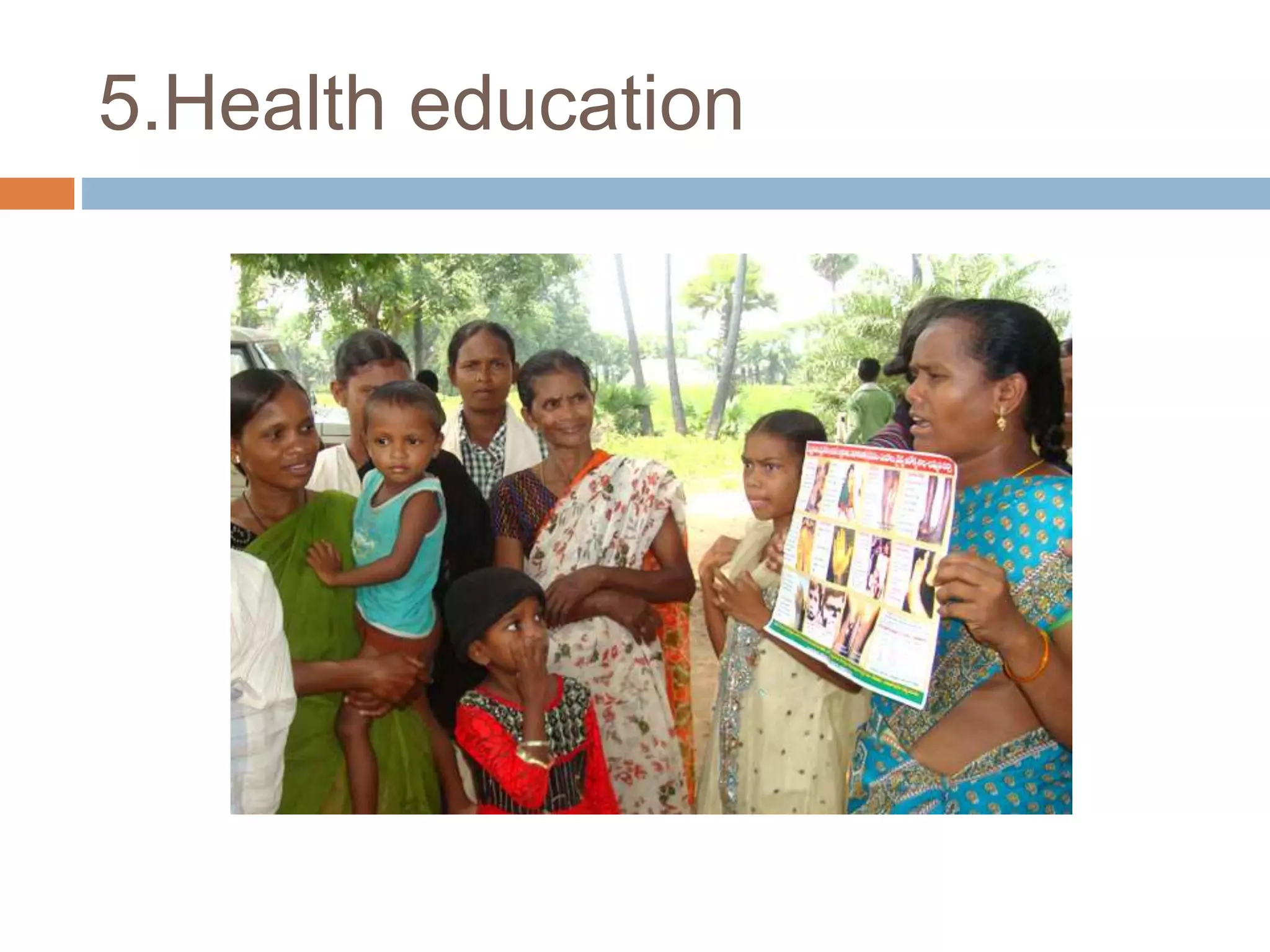

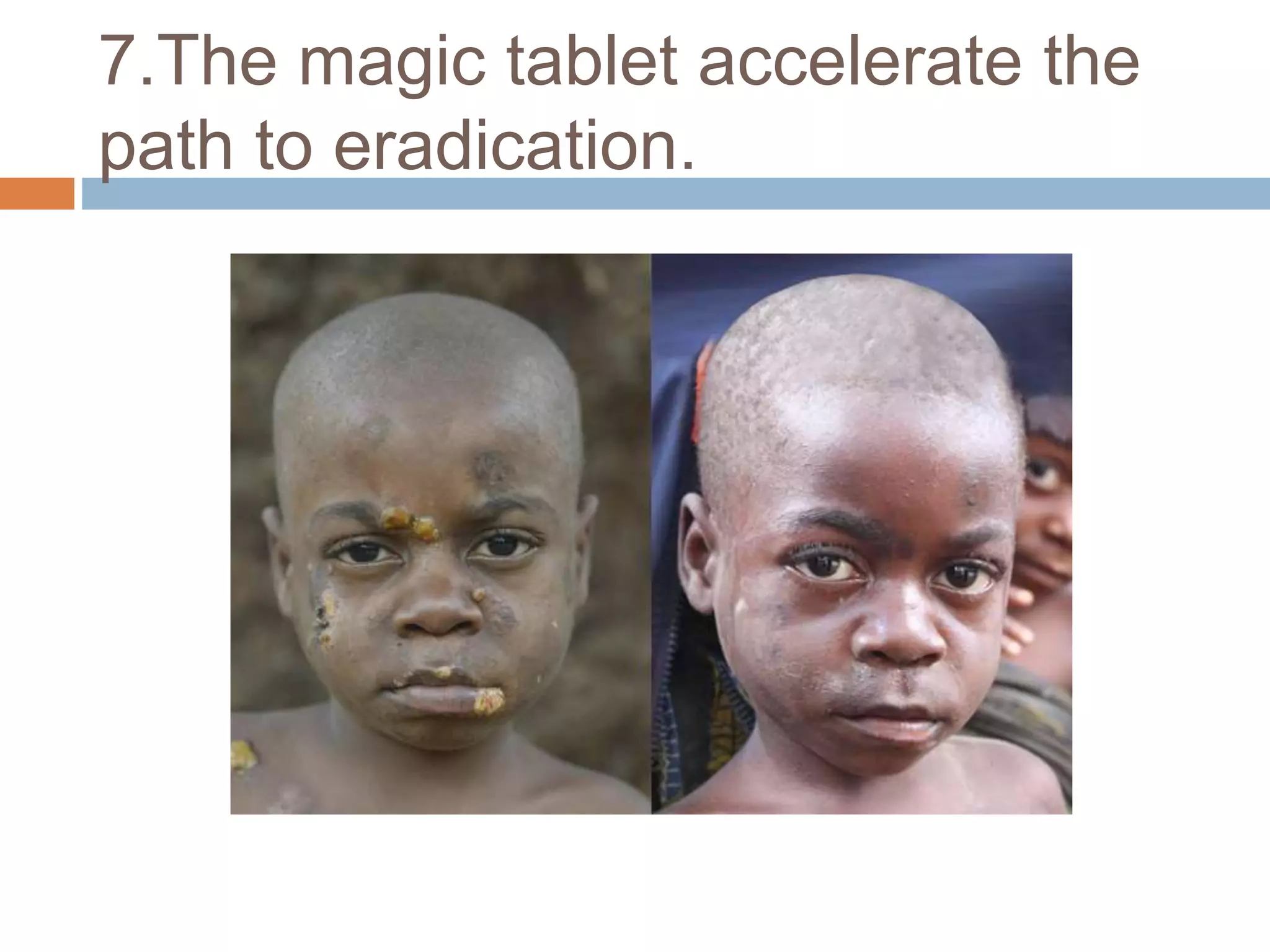
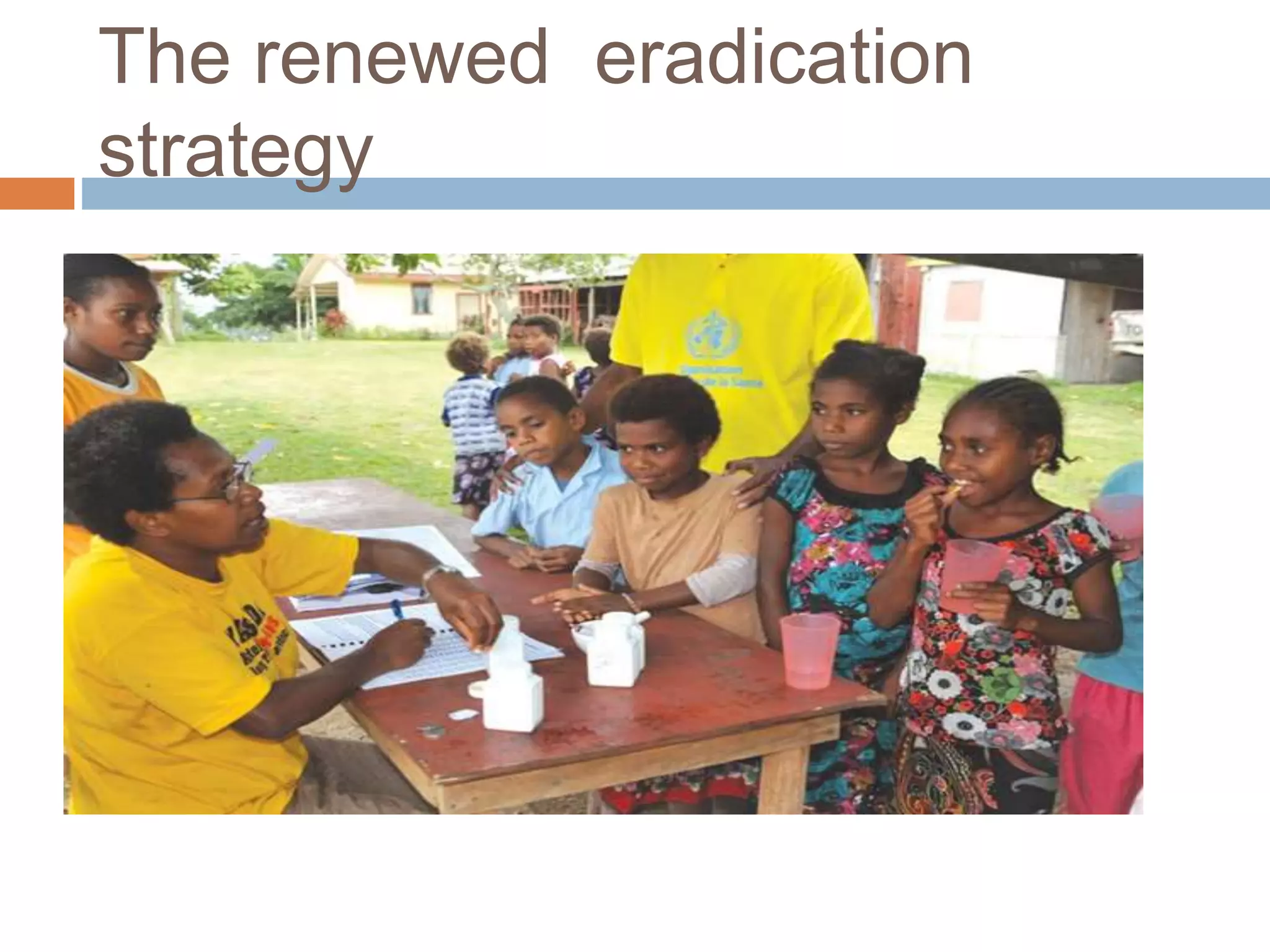

Yaws is a chronic bacterial infection that affects skin, bone, and cartilage, caused by Treponema pertenue. India launched a Yaws Eradication Programme in 1996-97, treating cases and contacts with antibiotics. Through surveillance and treatment, India declared elimination of yaws in 2006 and eradication in 2016, making it the first country certified by the WHO as free of yaws.


































































