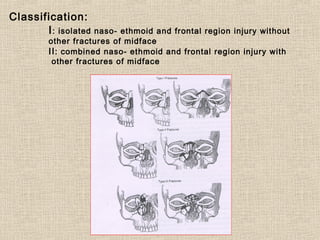
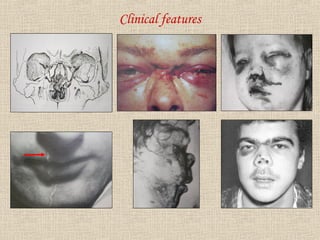
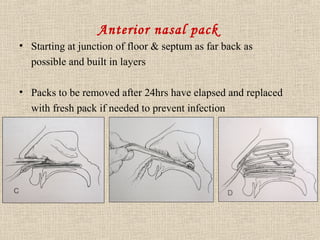
This document discusses nasoethmoidal fractures, which involve the nasal and ethmoid bones. It describes the anatomy of the nasoethmoid complex and classifies fractures. Clinical features include nasal deformity, frontal bone depression, cerebrospinal fluid leakage, hemorrhage, and diplopia. Diagnosis involves radiography and CT scans. Treatment involves reducing fractures, repairing dural tears causing CSF leakage, managing hemorrhage through cauterization or packing, and ensuring airway protection.