Downloaded 66 times




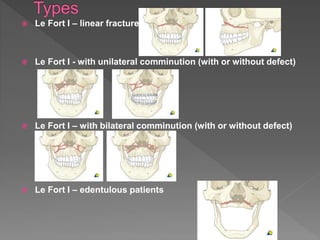
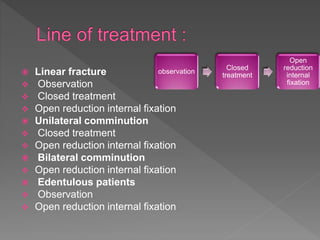
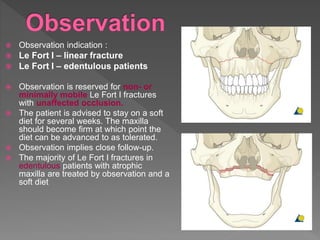
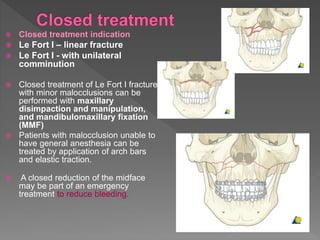
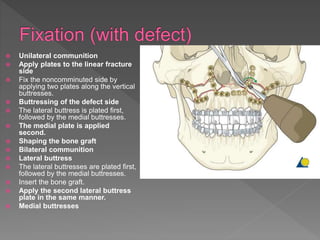
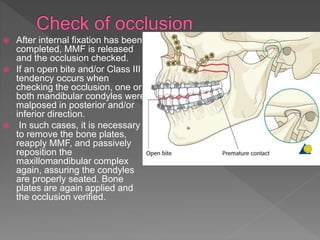


The document describes the classification and treatment of Le Fort I fractures. Le Fort I fractures can be linear, unilateral comminuted, or bilateral comminuted. Treatment depends on the classification and includes observation for non-mobile fractures, closed treatment for minor malocclusions, and open reduction internal fixation for more severe fractures. Open reduction involves exposing the fracture, reducing it, and fixing it with plates placed along the vertical buttresses of the maxilla. Bone grafting may be needed for defects. The occlusion is checked after fixation and corrected if needed.















































































