Downloaded 385 times

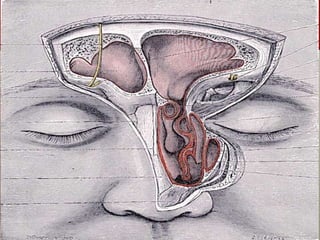
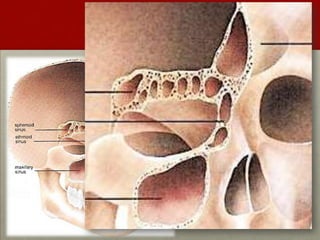
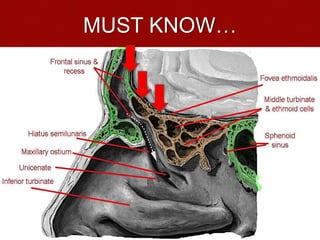
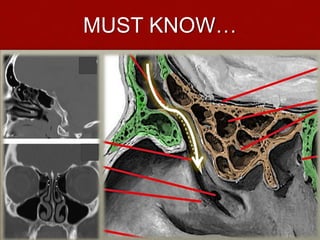

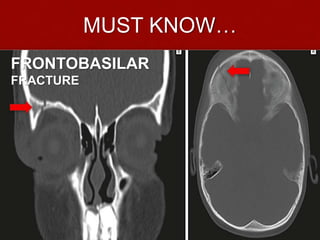




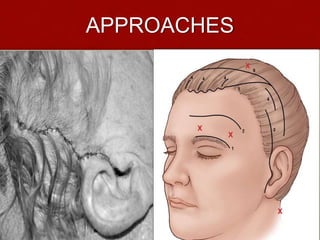

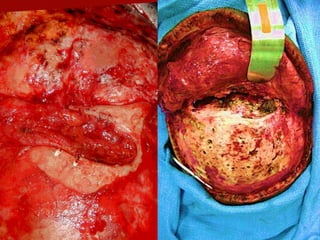

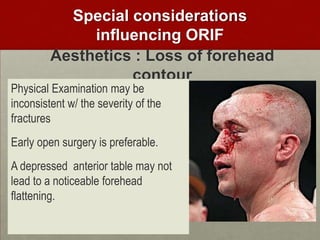
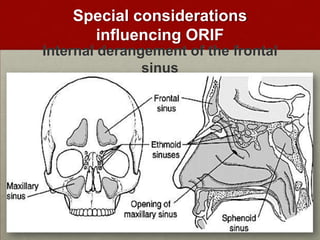
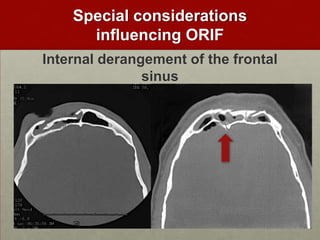
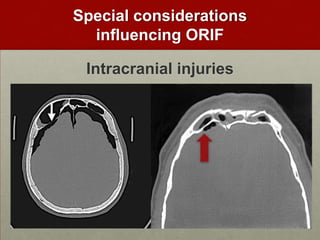
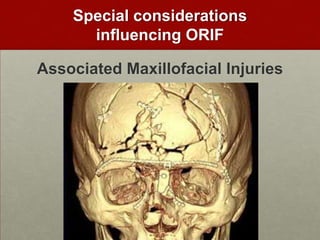

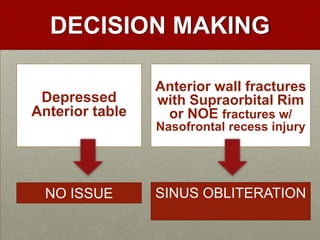
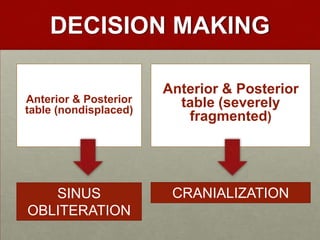
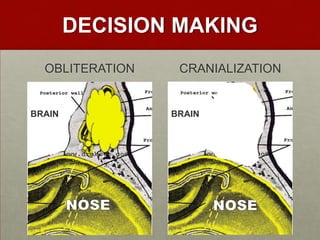
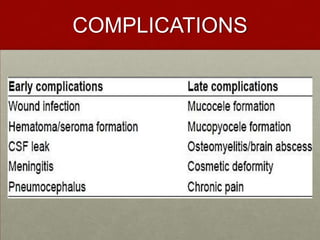

This document discusses frontal sinus fractures, including surgical anatomy, treatment approaches, considerations for open reduction and internal fixation (ORIF), and complications. It covers the anatomy of the olfactory bulb, cribriform plate, nasofrontal recess, and frontobasilar fractures that must be understood. Treatment goals are to restore facial contour and several surgical approaches are presented. Factors like intracranial injuries, other facial fractures, sinus derangement, and aesthetics can influence ORIF. Treatment may involve sinus obliteration or cranialization depending on fracture pattern. Perioperative care includes lumbar drains and antibiotics, though prolonged post-op antibiotics provide little benefit in preventing infections. Potential complications are also reviewed








































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


