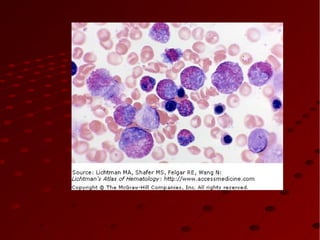
The document discusses myeloproliferative disorders (MPDs), which are clonal stem cell disorders characterized by increased blood cell counts and enlarged spleen and bone marrow. It focuses on chronic myeloid leukemia (CML), describing it as a MPD caused by a genetic mutation that results in uncontrolled white blood cell growth. CML progresses through chronic, accelerated, and blast phases, with symptoms ranging from fatigue to organ enlargement. Diagnosis involves blood and bone marrow tests detecting elevated white and platelet counts and the Philadelphia chromosome genetic abnormality associated with CML.


![Myeloproliferative DisordersMyeloproliferative Disorders
(2008 WHO classification)(2008 WHO classification)
1. polycythemia vera1. polycythemia vera
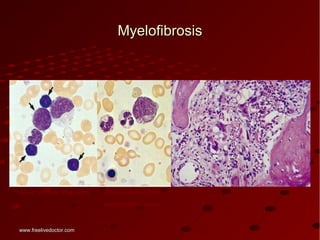
2. chronic idiopathic myelofibrosis2. chronic idiopathic myelofibrosis
3. essential thrombocytosis3. essential thrombocytosis
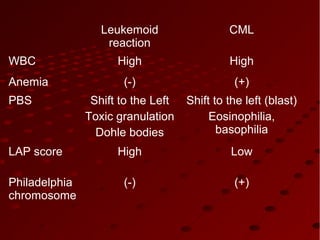
4. chronic myeloid leukemia (CML)4. chronic myeloid leukemia (CML)
5. [chronic neutrophilic leukemia]5. [chronic neutrophilic leukemia]
6. [chronic eosinophilic leukemia]6. [chronic eosinophilic leukemia]
7. [hypereosinophilic syndrome]7. [hypereosinophilic syndrome]
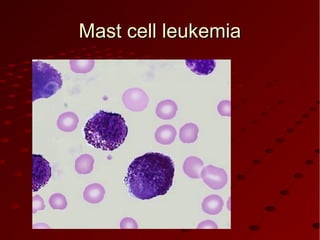
8.Mast cell disease8.Mast cell disease
““myelodysplastic/myeloproliferative diseases”myelodysplastic/myeloproliferative diseases”
juvenile myelomonocytic leukemiajuvenile myelomonocytic leukemia
atypical chronic myeloid leukemia (lacking t(9;22))atypical chronic myeloid leukemia (lacking t(9;22))
chronic myelomocytic leukemiachronic myelomocytic leukemia
www.freelivedoctor.comwww.freelivedoctor.com](https://image.slidesharecdn.com/myelo-130625011122-phpapp02/85/Myeloproliferative-disorders-4-320.jpg)




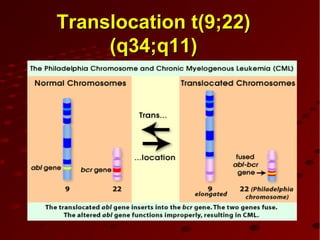
![PathogenesisPathogenesis
Genetic abnormalityGenetic abnormality
CML is the result of an acquired geneticCML is the result of an acquired genetic
abnormalityabnormality
A translocation between chromosome 9 andA translocation between chromosome 9 and
2222 [t(9;22)] – the[t(9;22)] – the Philadelphia chromosomePhiladelphia chromosome
The oncogene BCThe oncogene BCRR-ABL encodes an-ABL encodes an
enzyme – tyrosine phosphokinase (usuallyenzyme – tyrosine phosphokinase (usually
p210)p210)](https://image.slidesharecdn.com/myelo-130625011122-phpapp02/85/Myeloproliferative-disorders-11-320.jpg)