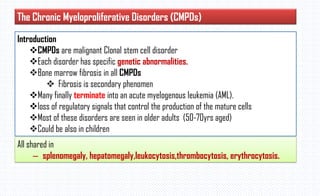
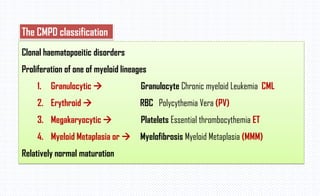
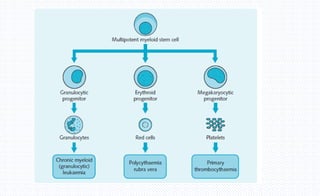
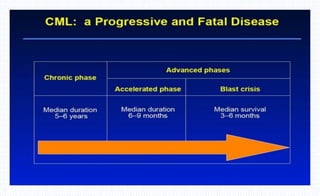
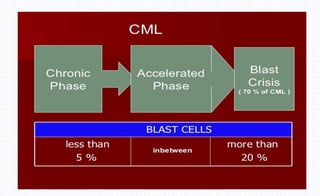
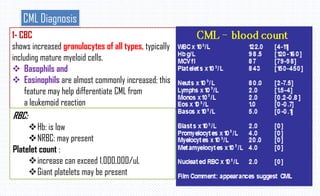
The document provides an overview of chronic myeloid leukemia (CML), a type of chronic myeloproliferative disorder characterized by increased granulocytic proliferation and linked to the Philadelphia chromosome translocation (t(9;22)). It outlines the disease course which progresses through three phases: chronic, accelerated, and blast crisis, with varying symptoms and survival rates at each stage. The document also details diagnostic features including hematological findings and the presence of specific genetic abnormalities.


![2-Bone Marrow study :
1-Cellularity: Hypercellular, Increase
reticulin fibrosis in 30-40%
2-Granulocytic hyperplasia blasts less
10%
3-Increase the M:E ratio
Myeloid:erythroid ratio – 10:1 to 30:1 (N :
2:1)
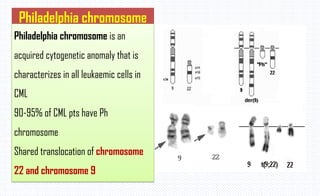
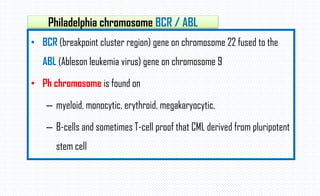
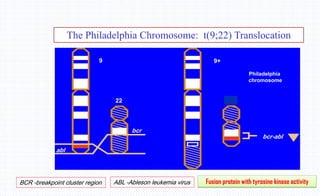
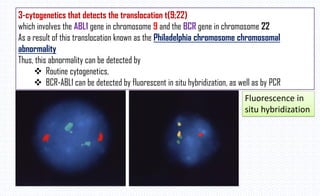
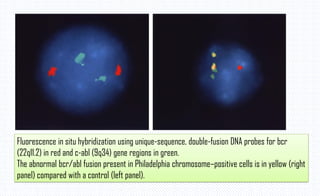
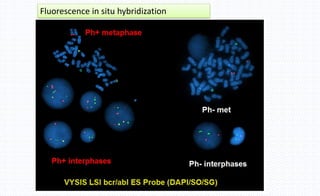
5-Ph.chromsome test: positive
[t(9;22)]
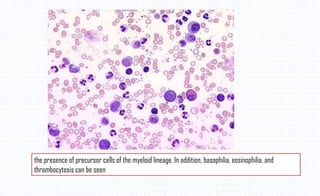
clear dominance of granulopoiesis. The number of eosinophils and
megakaryocytes is increased](https://image.slidesharecdn.com/cml-230220104658-e06c2a53/85/CML-pdf-19-320.jpg)

















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















