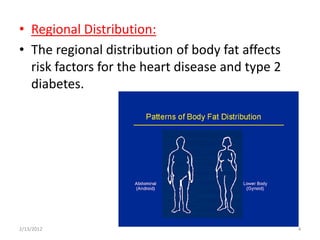
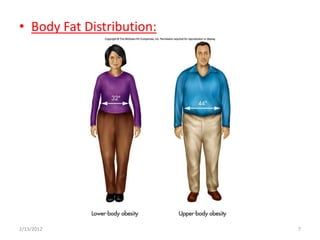
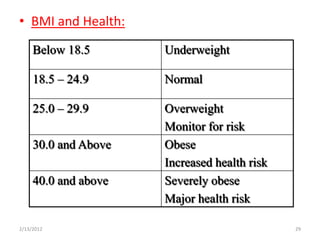
The document discusses obesity, defining it as excessive body fat over 35% for women and 25% for men. It outlines the health risks of obesity like heart disease, diabetes, and certain cancers. Factors that contribute to obesity are discussed, like overeating high calorie foods, sedentary lifestyles, genetics, and certain medical conditions. Regional fat distribution is important, with abdominal fat posing more risks than lower body fat. The document provides guidelines for measuring obesity through BMI and outlines treatments like diet, exercise and medication or surgery in severe cases.