This document discusses neutrophilic dermatoses, a spectrum of disorders characterized by neutrophilic infiltration of the skin without true vasculitis. Key points include:
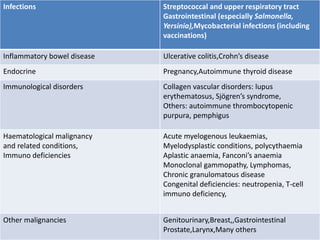
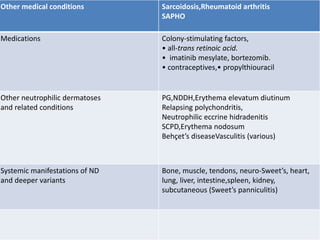
- Common features include a neutrophilic vascular reaction, some cases having a reactive or systemic cause, disorders may coexist or occur sequentially in individuals.
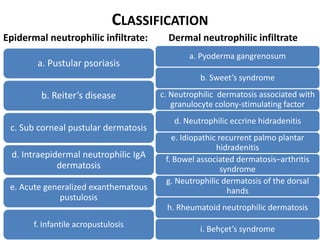
- Classification includes disorders grouped by location of neutrophilic infiltrate (epidermal vs dermal).
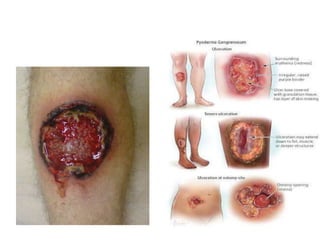
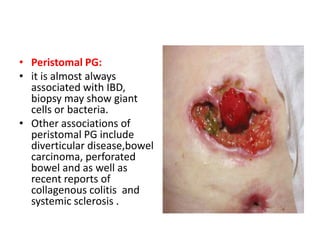
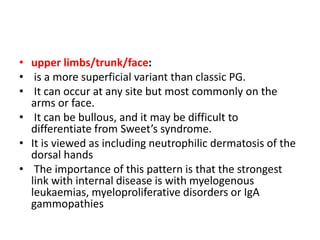
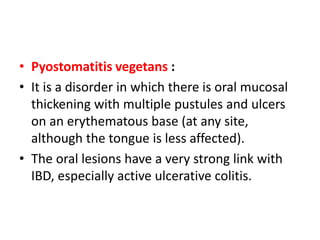
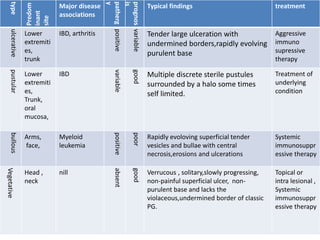
- Pyoderma gangrenosum is discussed in depth, including its pathogenesis, associated diseases, diagnostic criteria, variants (classic, pustular, bullous etc.), investigations and histopathology. Treatment involves immunosuppressive therapy.

















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















