This document presents a case report of a newborn with multicystic dysplastic kidney (MCDK). The key points are:
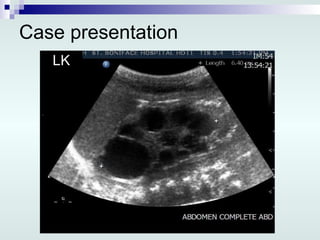
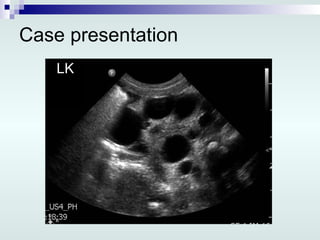
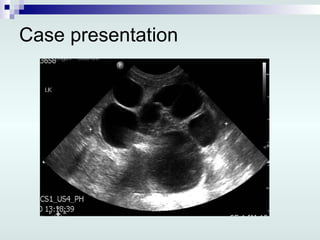
1) Prenatal ultrasound identified a cystic enlargement of the left kidney in the fetus.
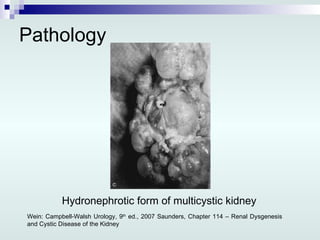
2) After a preterm delivery, examination of the newborn found generalized edema, dysmorphic features, and a grossly edematous left MCDK.
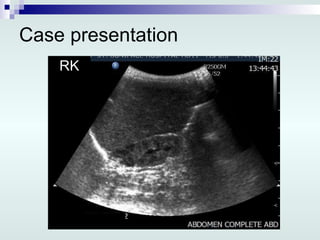
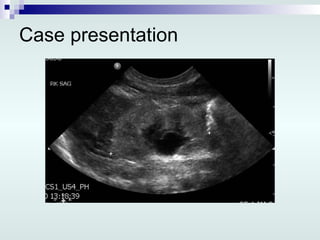
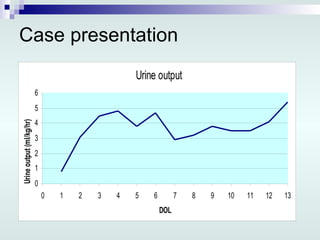
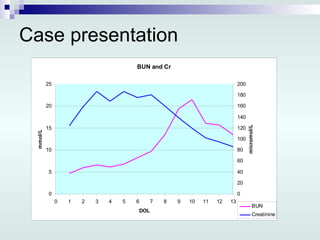
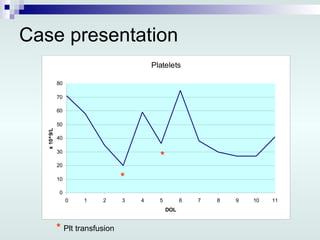
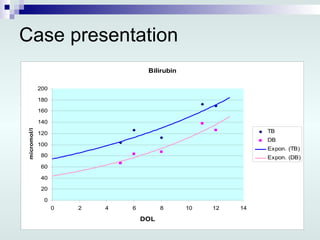
3) Workup revealed renal failure. Imaging showed a small right kidney. The newborn was treated with peritoneal dialysis.














































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















