The document discusses neonatal infection risks associated with prolonged rupture of membranes and strategies for prevention and management. Key points:
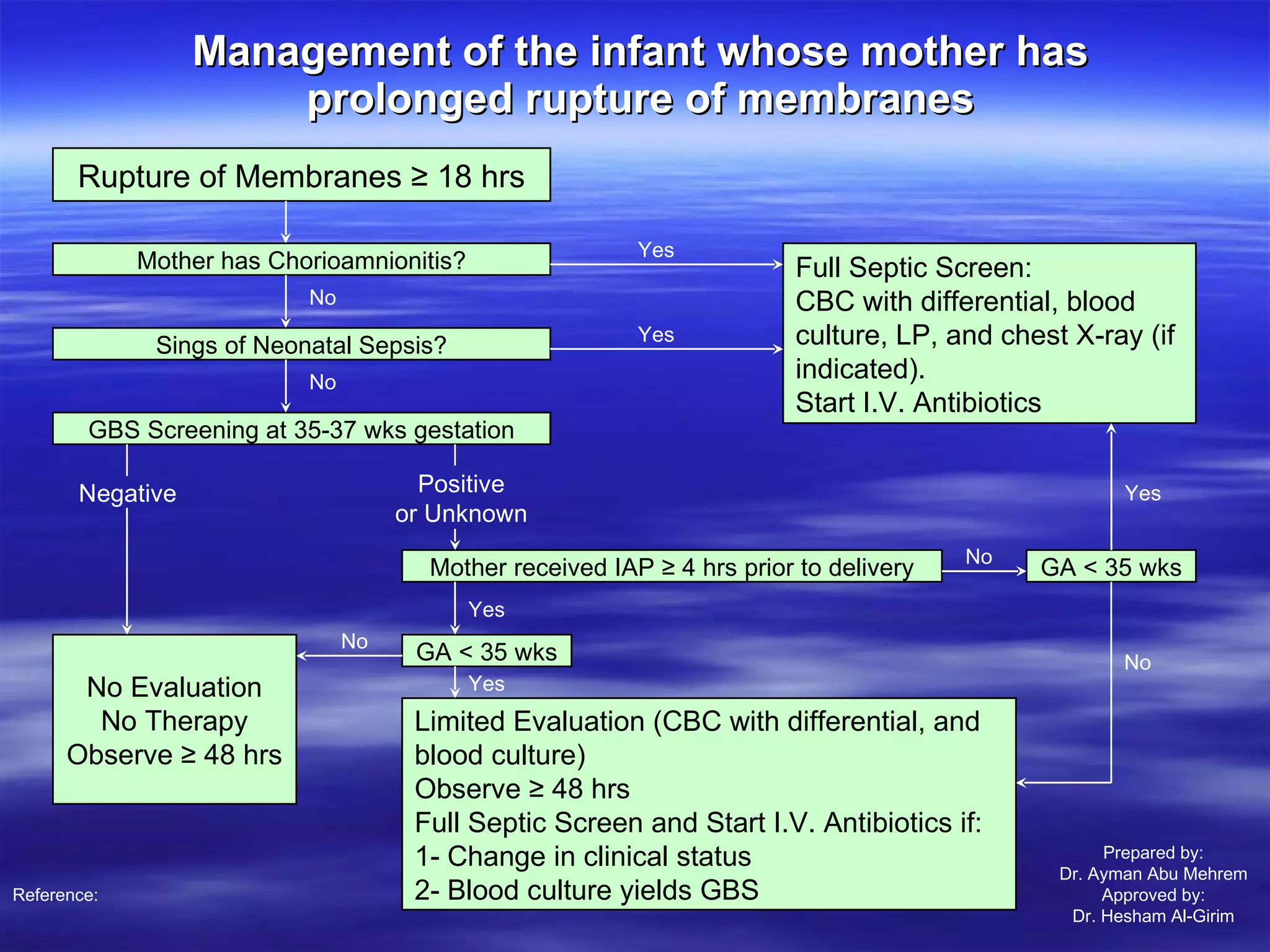
- Rupture of membranes for longer than 18 hours increases the risk of chorioamnionitis and neonatal infection due to ascending bacterial infection from the birth canal.
- Preterm infants have higher infection risks due to immune dysfunction and invasive procedures.
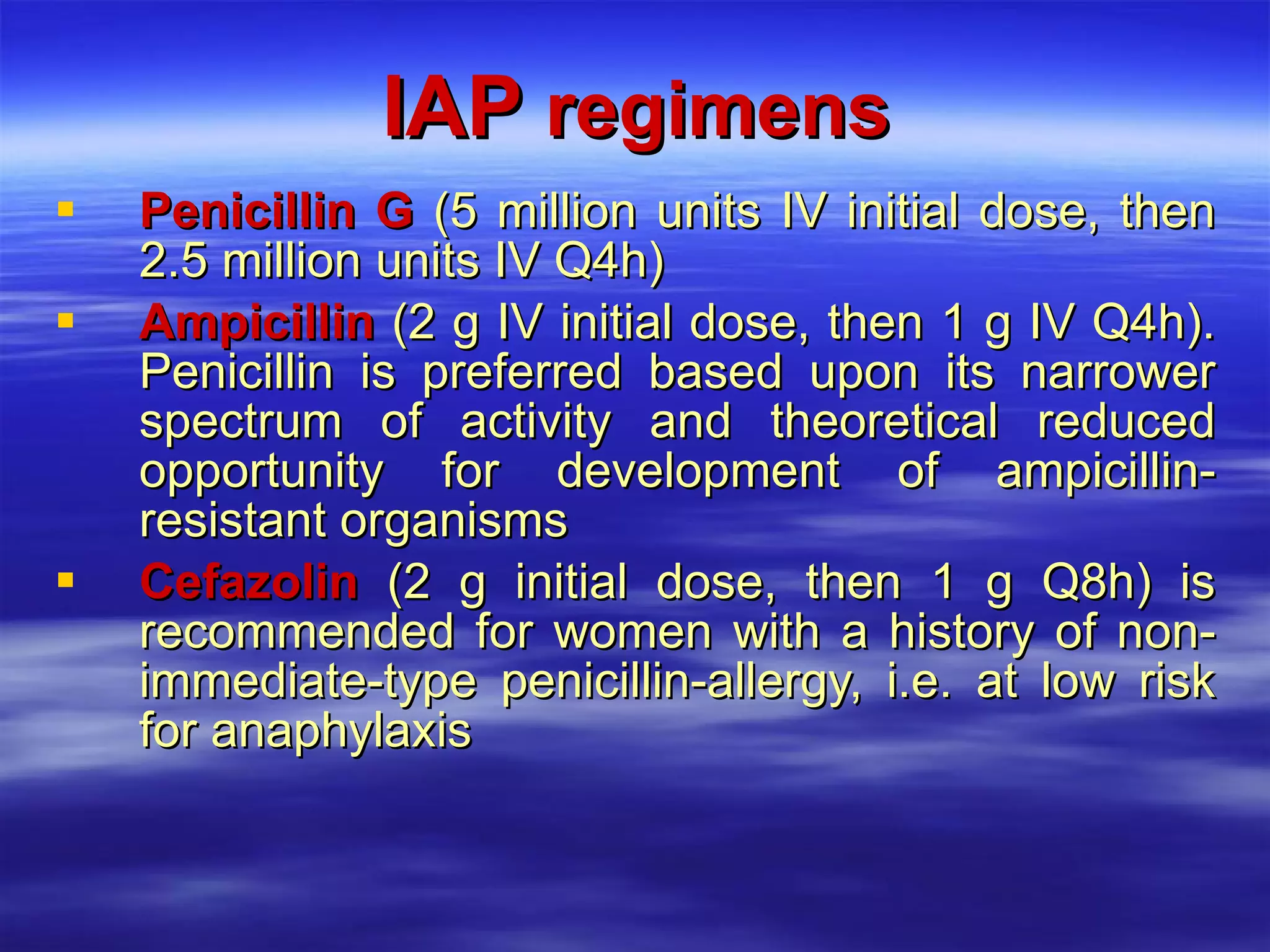
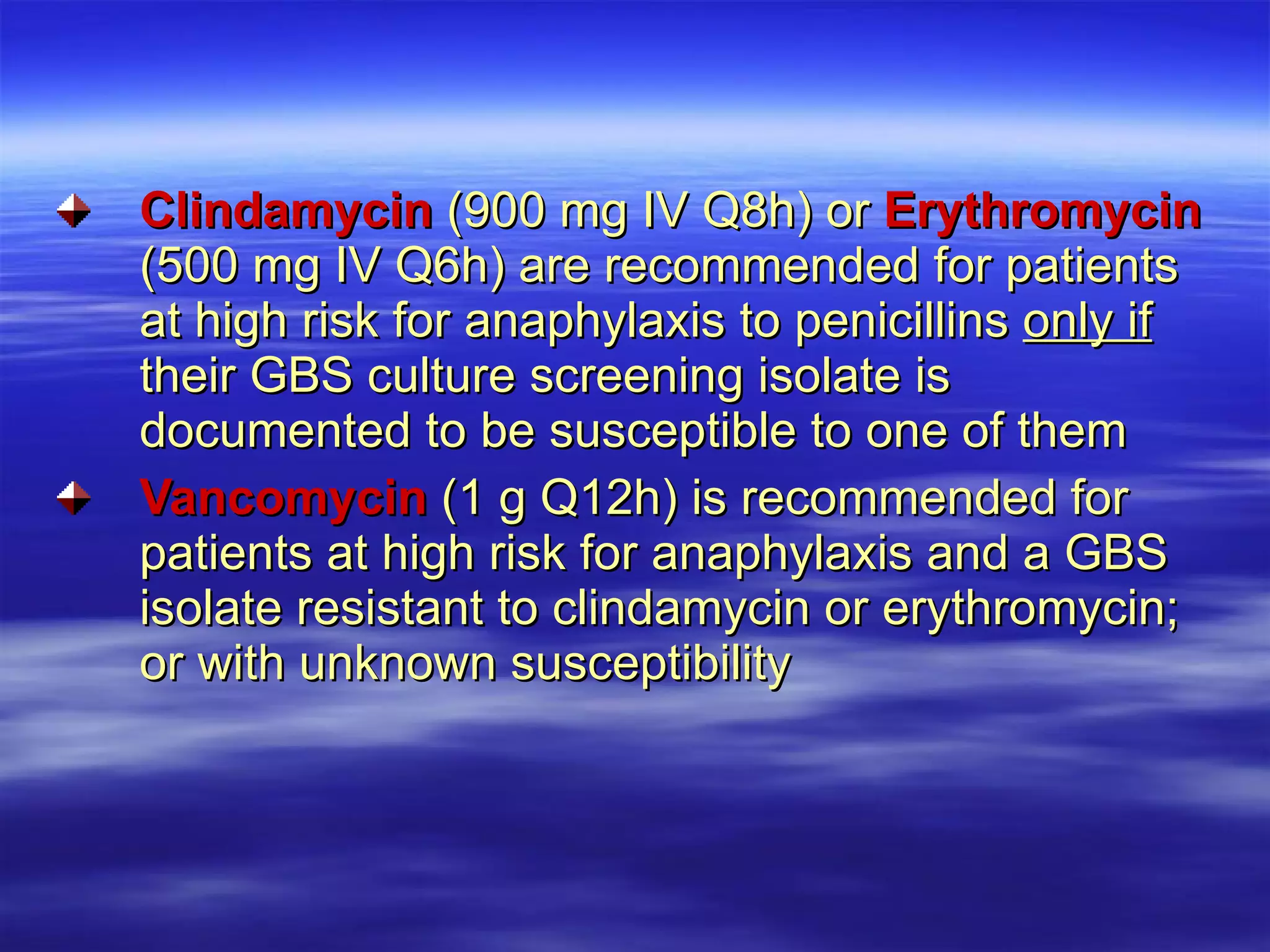
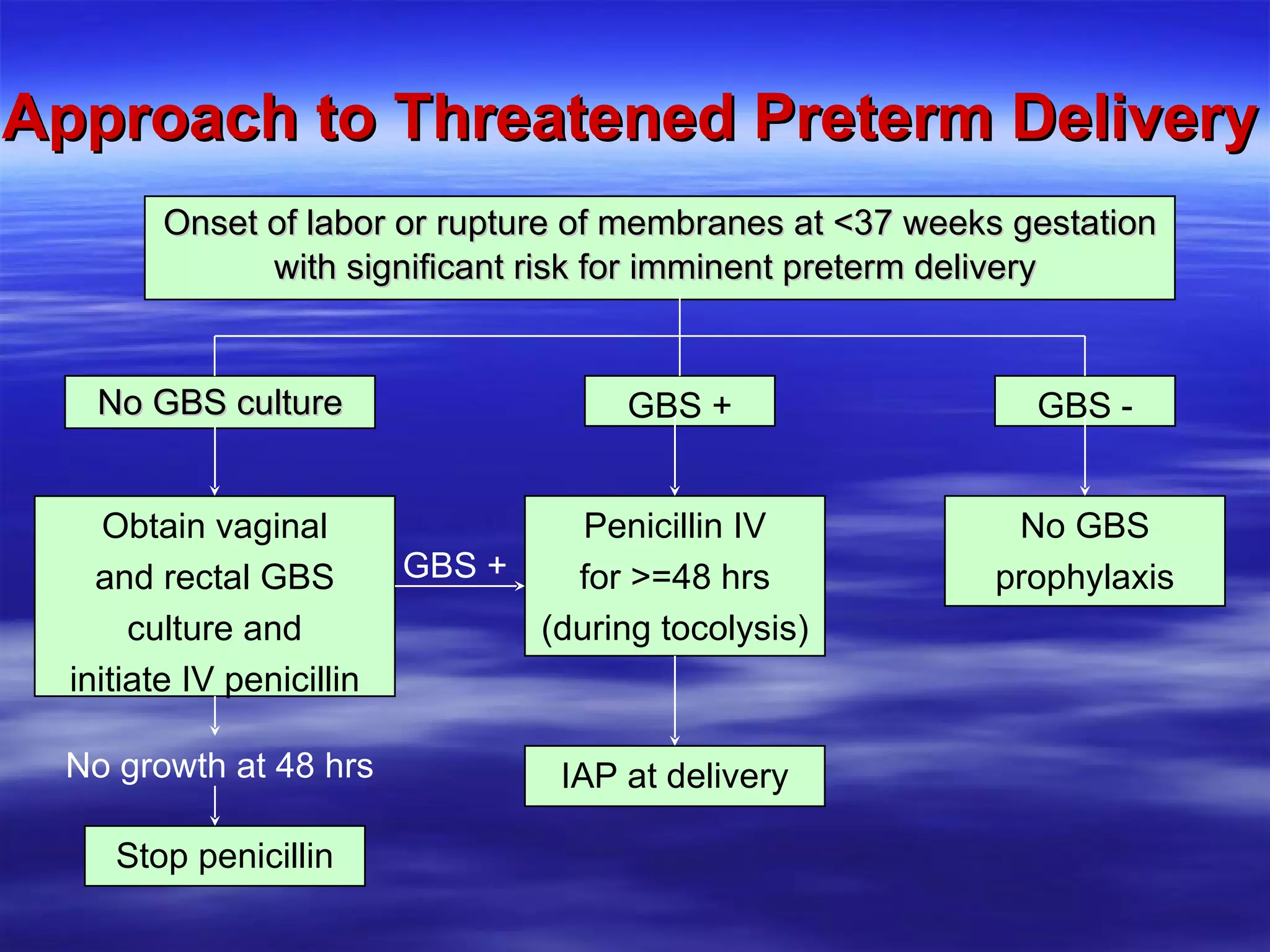
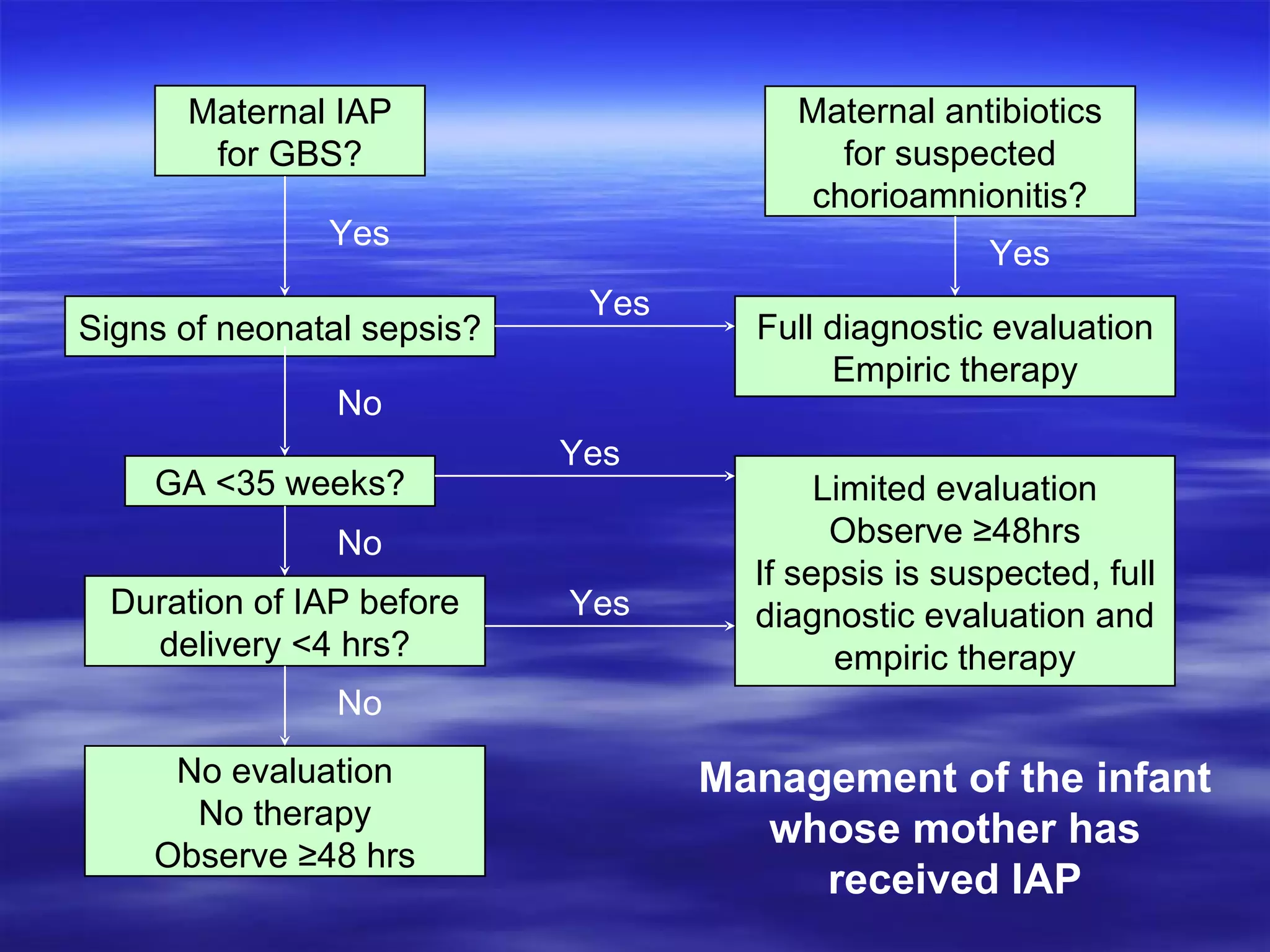
- Guidelines recommend screening all pregnant women for Group B Streptococcus (GBS) at 35-37 weeks and administering intrapartum antibiotics (IAP) for those who test positive or have other risk factors.
- Management of infants involves observation and/or limited evaluation and empiric antibiotics depending on gestational age,































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






