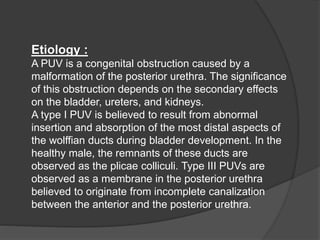
Posterior urethral valves are congenital obstructions of the urethra that commonly cause urinary tract obstruction in boys. They develop from abnormal remnants of the wolffian duct during early bladder development. Presentation is usually prenatal due to hydronephrosis seen on ultrasound. Long term risks include renal dysfunction and end stage renal disease due to damage from high pressures in the urinary tract. Management involves early surgical removal of the valves and lifelong monitoring of kidney and bladder function.

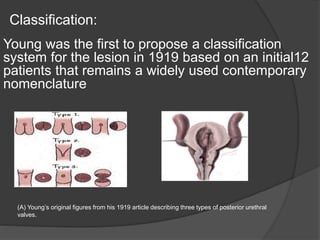
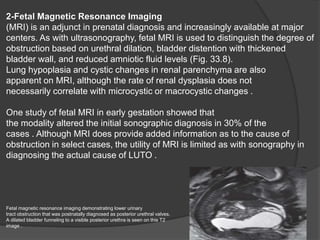
![Imaging Studies:
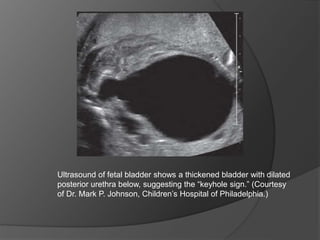
Ultrasonography
Antenatal ultrasonography (US) has been found to be reasonably accurate in
distinguishing PUV from vesicoureteral reflux (VUR).
Every child with antenatal hydronephrosis should be assessed with renal
and bladder US in the immediate postnatal period,[17]with a focus on the
appearance of the renal parenchyma, any evidence of renal collecting
system dilatation, the thickness of the bladder wall, and the presence or
absence of ascites. The quantity (total area) and quality (corticomedullary
differentiation and renal echogenicity) of the renal parenchyma on initial
postnatal US have prognostic value for determining the future risk of stage 5
chronic kidney disease.
Because newborns commonly have relative hypovolemia during the first few
days of life, it is recommended to perform US after the first week of life if
findings from the first US examination were normal in a child with previously
diagnosed antenatal hydronephrosis before making a final determination that
the hydronephrosis has resolved .
Contrast-enhanced serial voiding urosonography has been sugegsted as a
useful complementary test in pediatric patients with PUVs.](https://image.slidesharecdn.com/puvdrosamalmogahed-231025151326-ea83c82f/85/Posterior-urethral-valve-28-320.jpg)
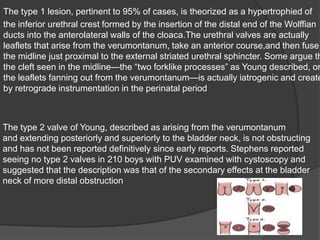
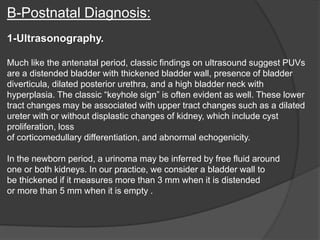
![Procedures:
Cystoscopy serves both diagnostic and therapeutic functions in these infants.
Appropriately-sized cystoscopes (< 8 French) are needed to avoid injury to the
urethra.
**Diagnostic
Confirmation with cystoscopy is required in every child in whom PUV is
suggested after VCUG. In some, the filling defect observed on VCUG may
represent only external sphincter contraction during voiding; in others, the valve
leaflets are confirmed.
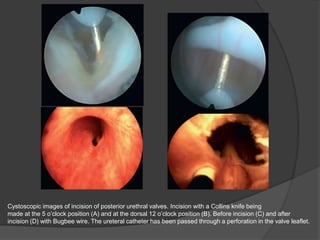
**Therapeutic (ie, transurethral incision of PUVs)
Multiple techniques are described for PUV ablation. Disruption of the
obstructing membrane by blind passage of a valve hook is now only of historic
interest. Currently, valves are disrupted under direct vision by cystoscopy using
an endoscopic loop, Bugbee electrocauterization, or laser fulguration. In
extremely small infants (< 2 kg), a 2-French Fogarty catheter may be passed
either under fluoroscopic or direct vision for valve disruption.[21]This is
performed in the least traumatic fashion possible to avoid secondary urethral
stricture or injury to the urethral sphincter mechanism.](https://image.slidesharecdn.com/puvdrosamalmogahed-231025151326-ea83c82f/85/Posterior-urethral-valve-30-320.jpg)

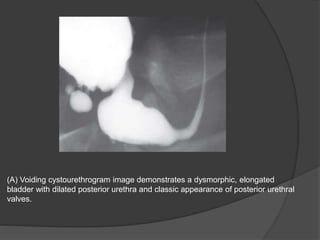
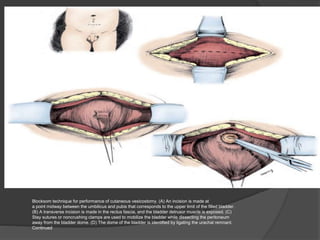
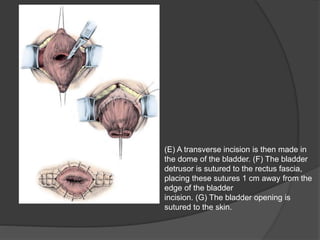
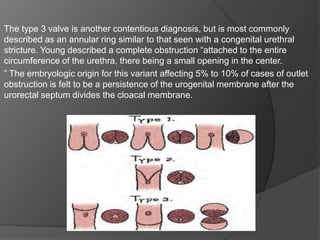
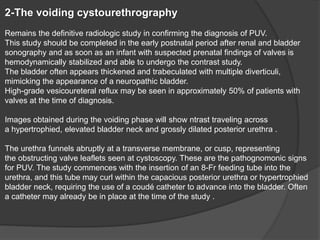
![Bladder dysfunction:
All male children with antenatal hydronephrosis should undergo voiding
cystourethrography (VCUG) shortly after birth to exclude PUV. While the study results are
being awaited, a 5- or 8-French urethral catheter should be placed to allow for bladder
drainage. If valves are confirmed, they can be incised within the first few days of life.
However, the newborn urethra may be too small to accommodate available equipment. In
these individuals, a vesicostomy can be performed as a temporary solution until urethral
growth has been adequate to allow transurethral incision.
Secondary ureterovesical junction obstruction from bladder hypertrophy is a controversial
issue. Supravesical urinary diversion procedures (eg, cutaneous ureterostomies) are
reserved for patients who appear to have ureterovesical junction obstruction. This is very
uncommon.
Later in childhood, severe or prolonged urethral obstruction can lead to a fibrotic, poorly
compliant bladder. This occurs when the developing bladder is exposed to high pressures
from bladder outlet obstruction, leading to increases in bladder collagen deposition and
detrusor muscle hypertrophy and hyperplasia. These bladders manifest poor compliance,
leading to elevated storage pressures. This, in turn, leads to increased risk of reflux,
hydroureteronephrosis, and urinary incontinence.
Use of urodynamic testing to assess bladder compliance helps identify patients at risk.
Some patients may respond to anticholinergic medication, such as oxybutynin.[25, 26,
27]Institution of clean intermittent catheterization (CIC) may aid some patients in
achieving continence by preventing the bladder from overfilling. In patients who do not
gain adequate bladder capacity and safe compliance despite optimal medical
management, augmentation cystoplasty may be required.](https://image.slidesharecdn.com/puvdrosamalmogahed-231025151326-ea83c82f/85/Posterior-urethral-valve-37-320.jpg)